General Information
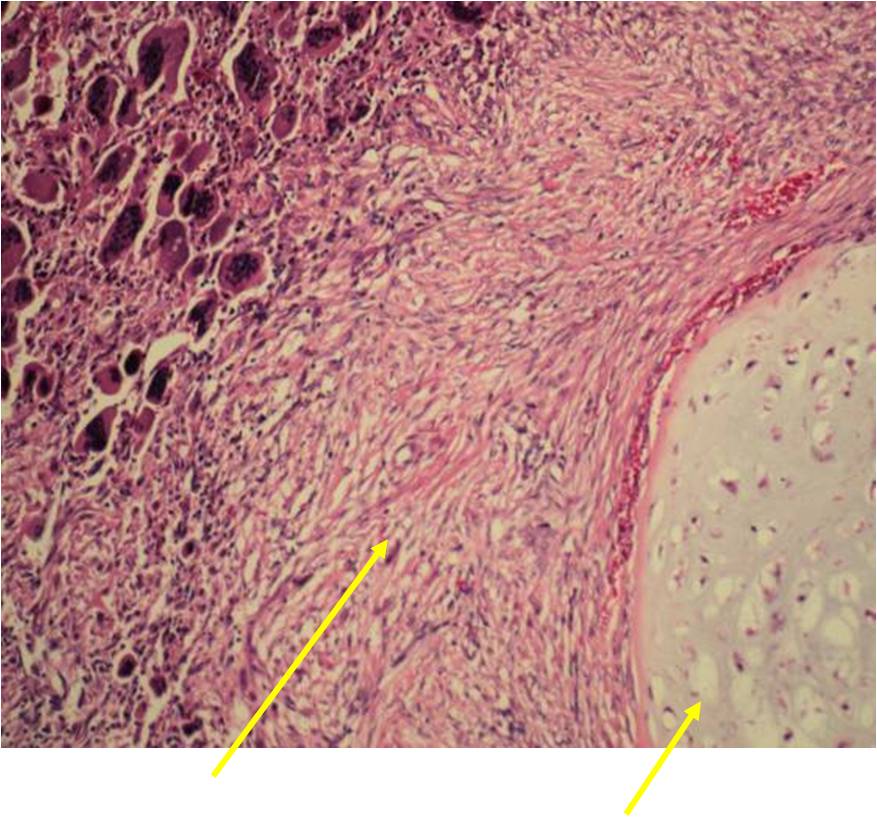
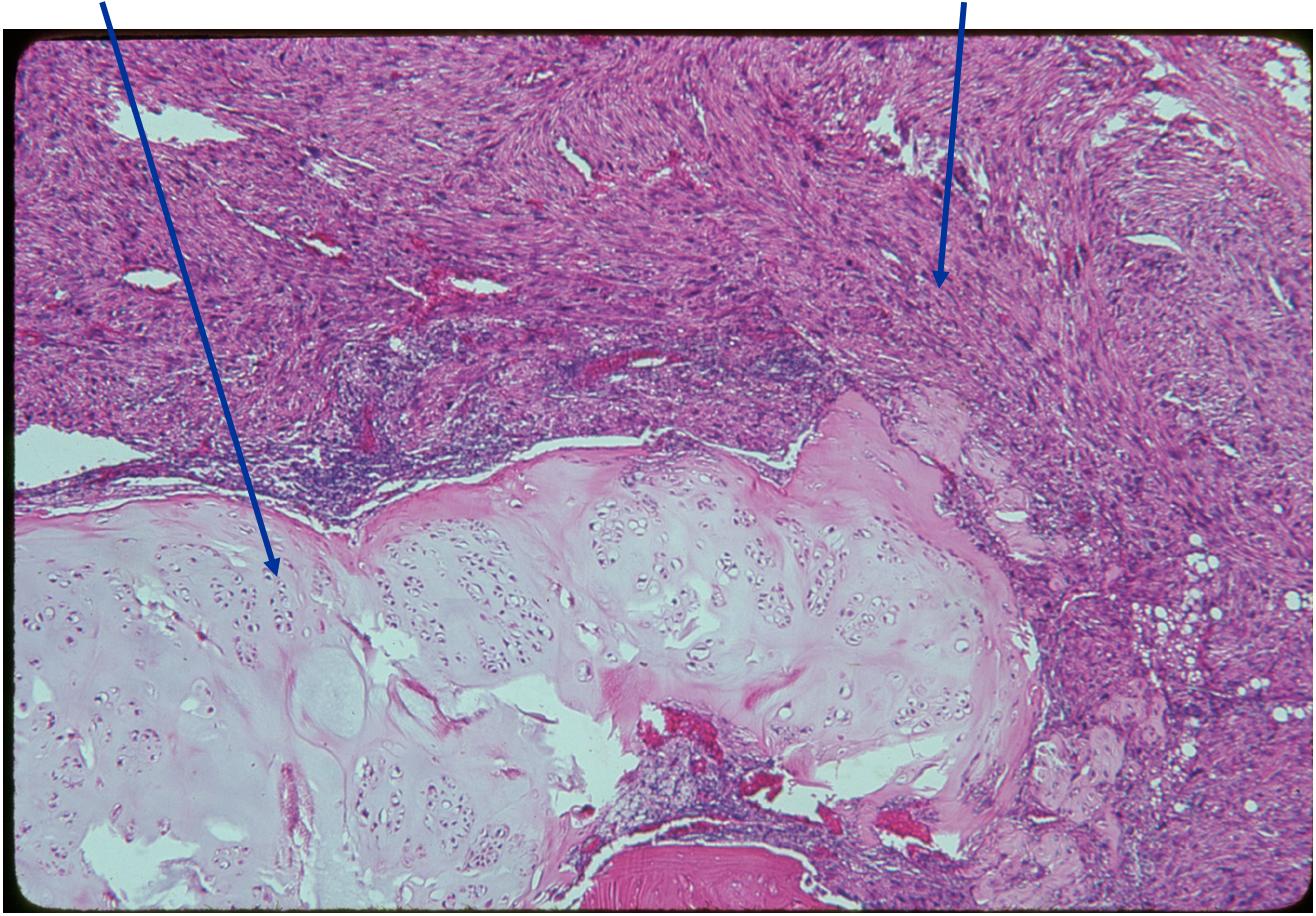
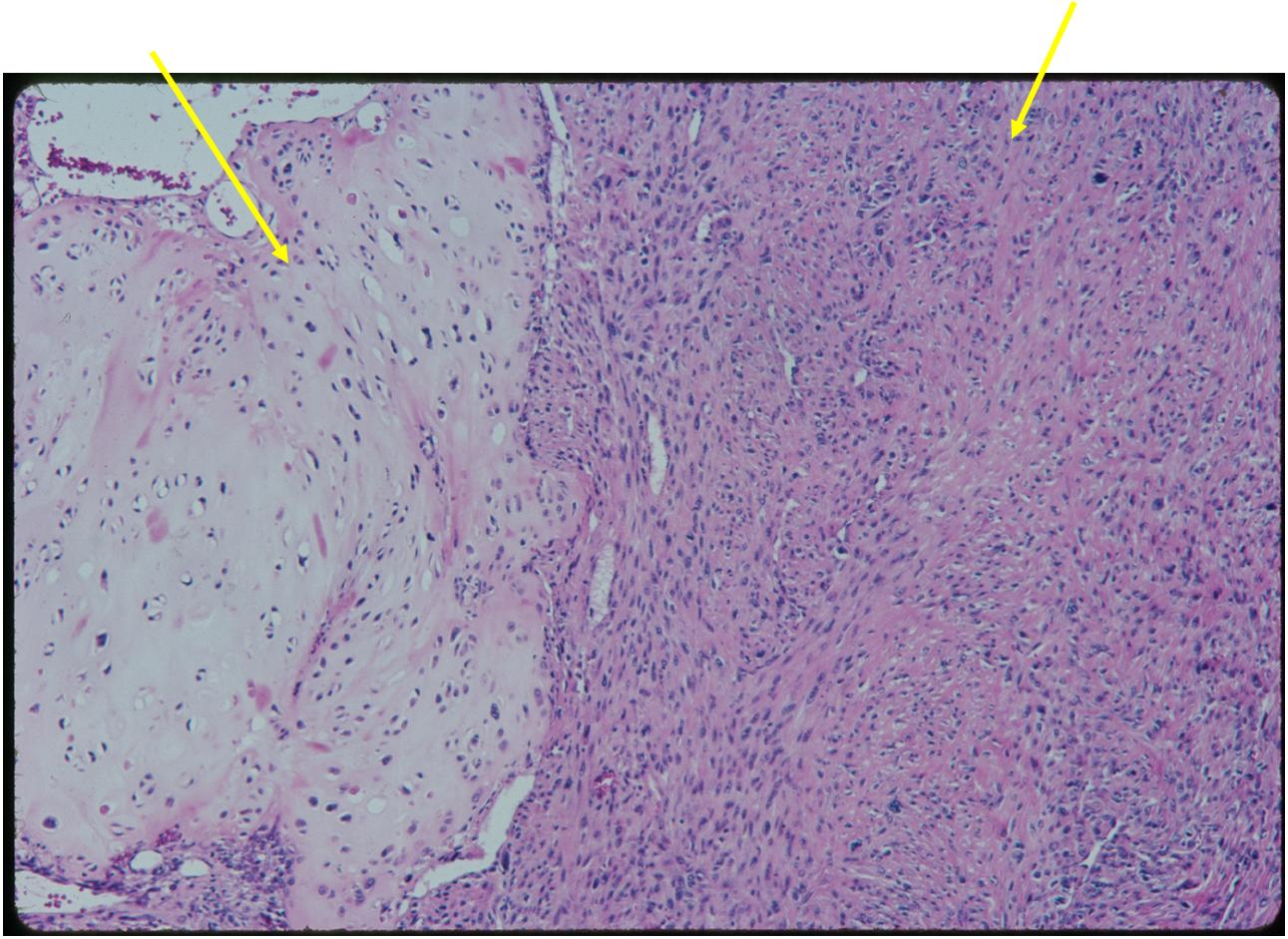
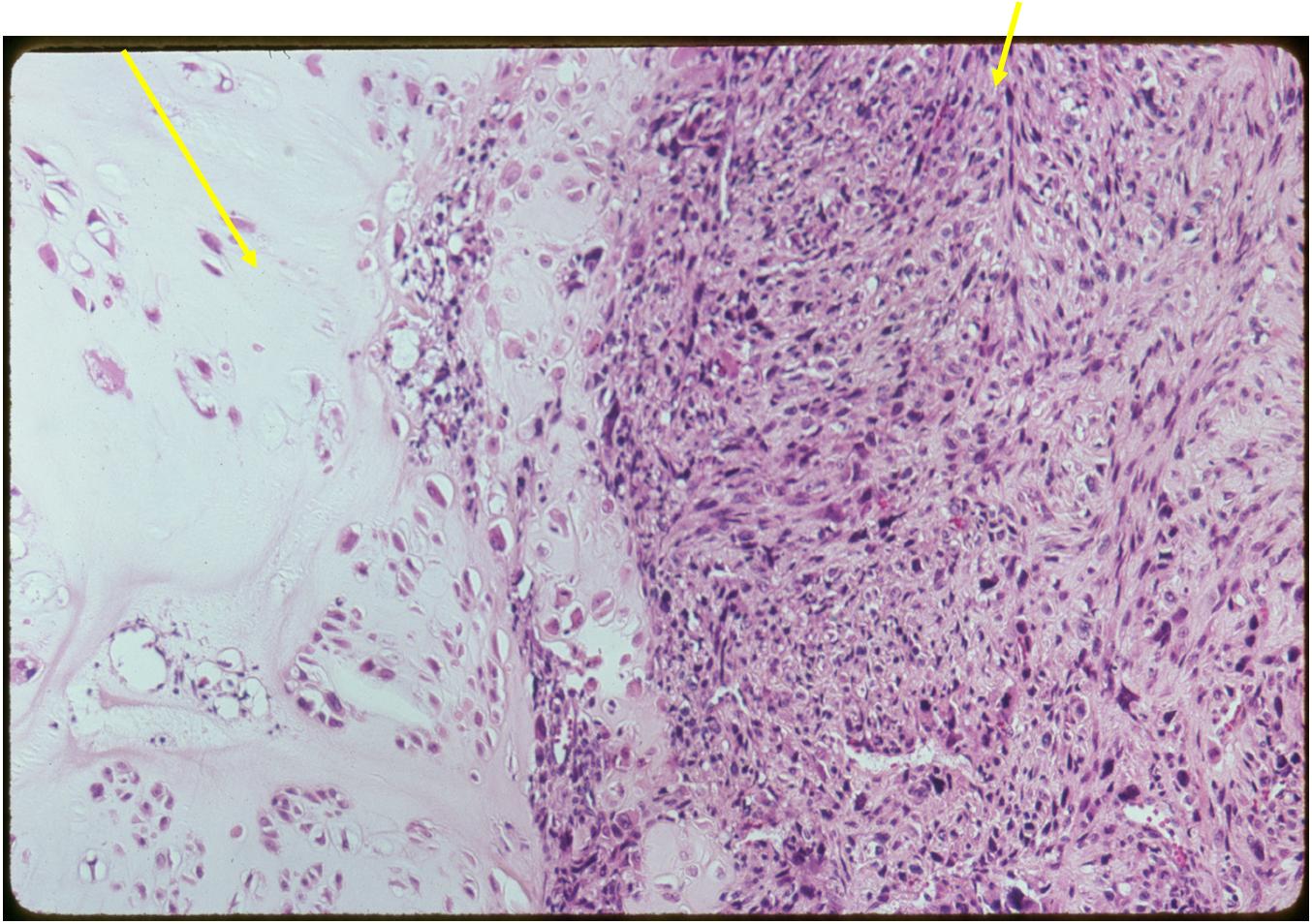
Dedifferentiated chondrosarcoma consists of a low grade malignant hyaline cartilage tumor associated with a high-grade nonchondroid spindle sarcoma. The two components are juxtaposed with abrupt clear demarcation line
- The high grade sarcoma is most commonly an MFH, osteosarcoma or fibrosarcoma although others may occur
- It is an extremely aggressive tumor with a high metastatic rate and dismal prognosis
- Constitutes approximately 10% of chondrosarcomas
- 50% arise from a secondary chondrosarcoma
Clinical Presentation
Signs/Symptoms:
- Pain, with or without pathological fracture
- Swelling
- Parasthesias
- Symptoms usually last around 6-10 months
Prevalence:
- 11% of all chondrosarcomas
- No predilection for sex or race
Age:
- Young adulthood to old age
- Most patients are older than 50
Sites:
- Most common in pelvis, proximal femur, proximal humerus, distal femur, ribs
- Similar sites as conventional chondrosarcoma
Radiographic Presentation
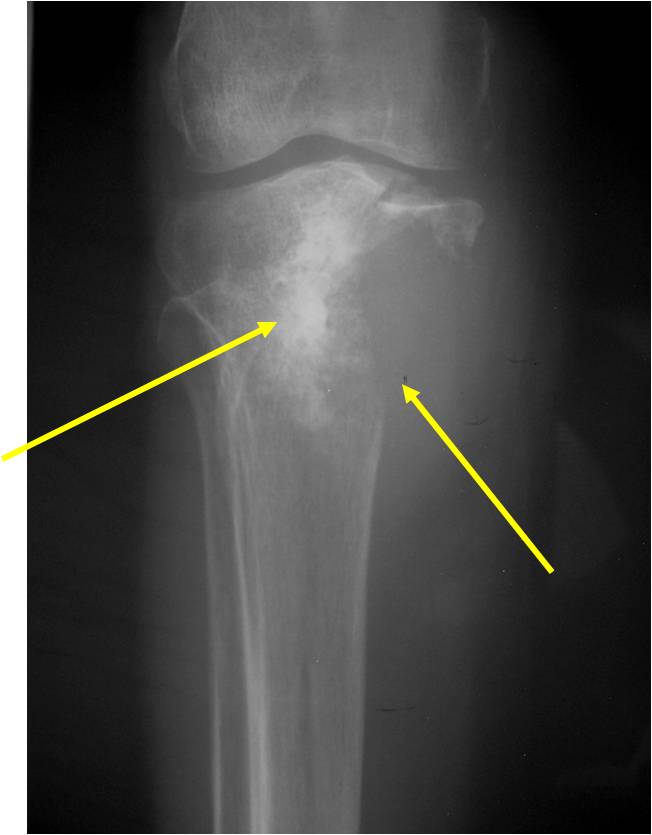
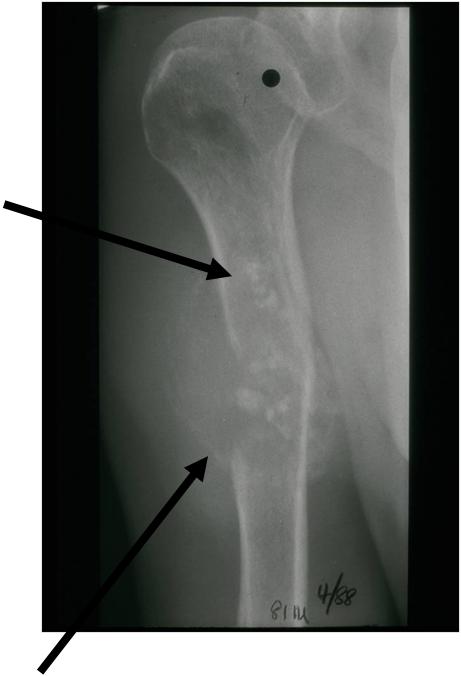
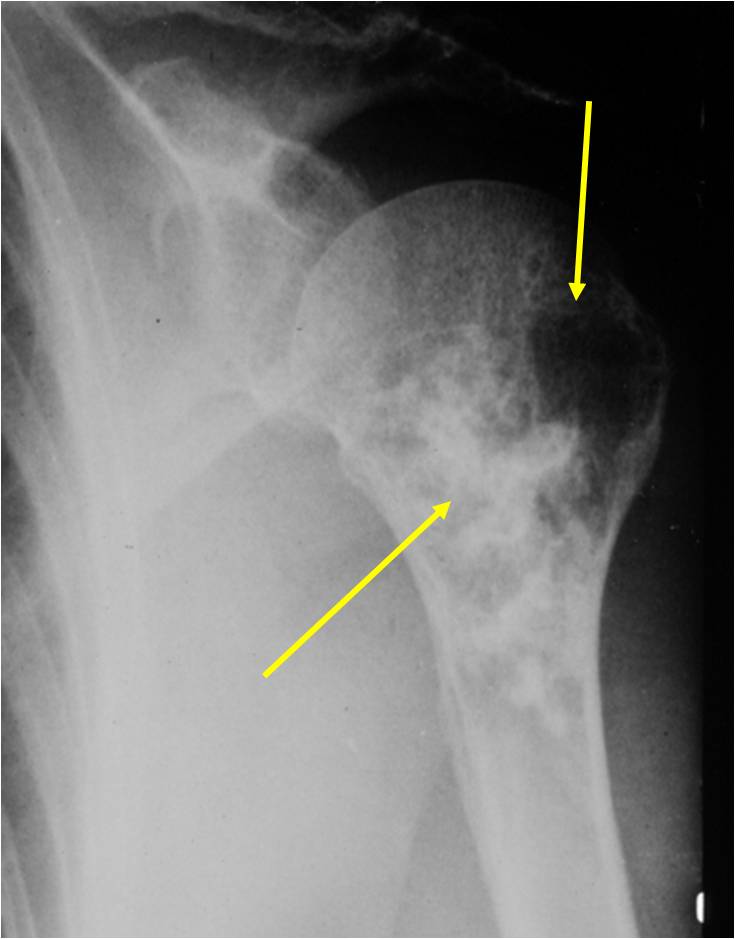
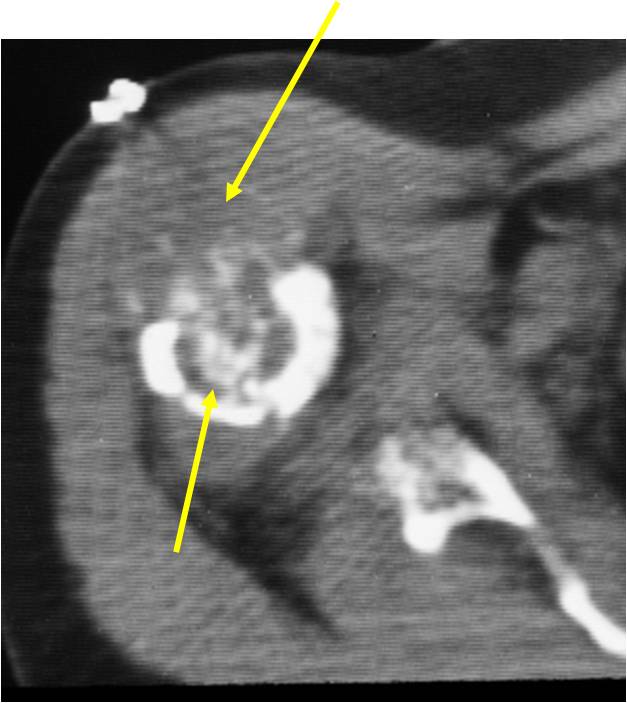
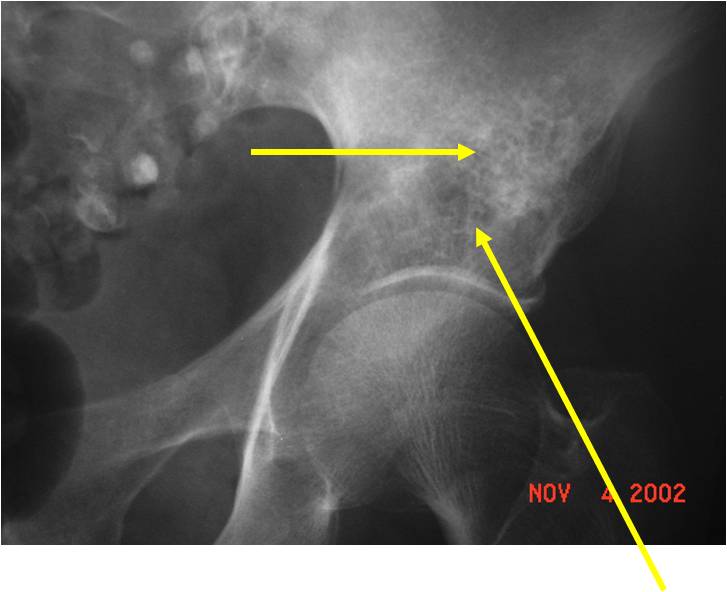
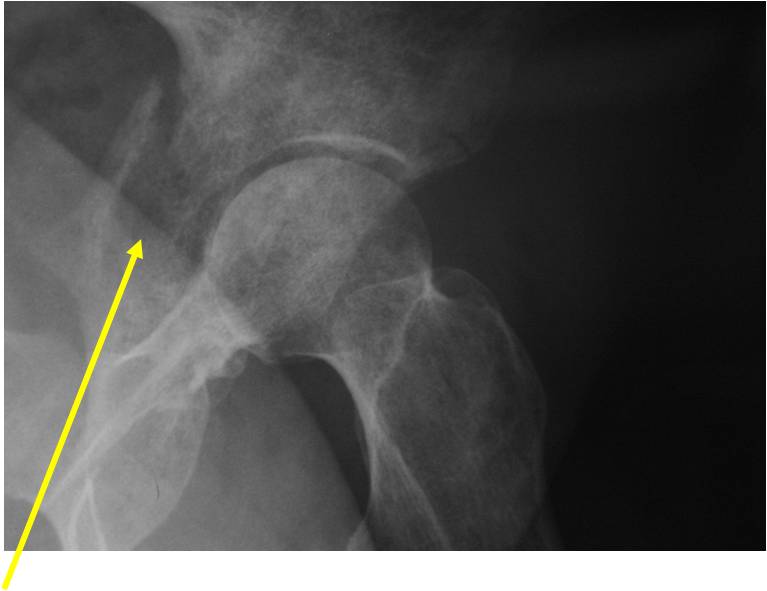
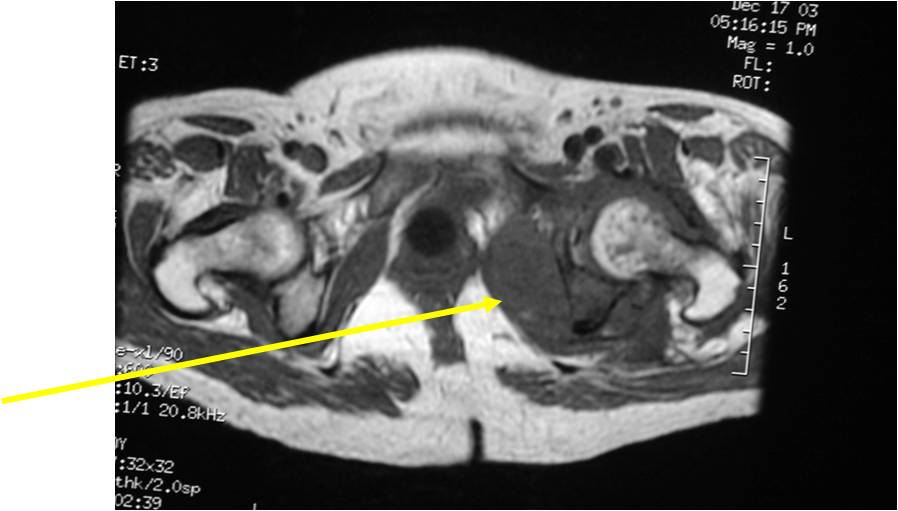
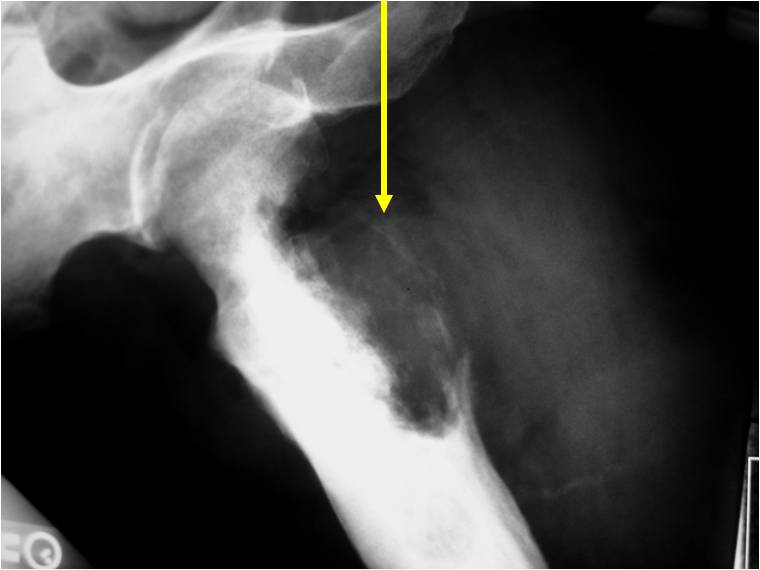
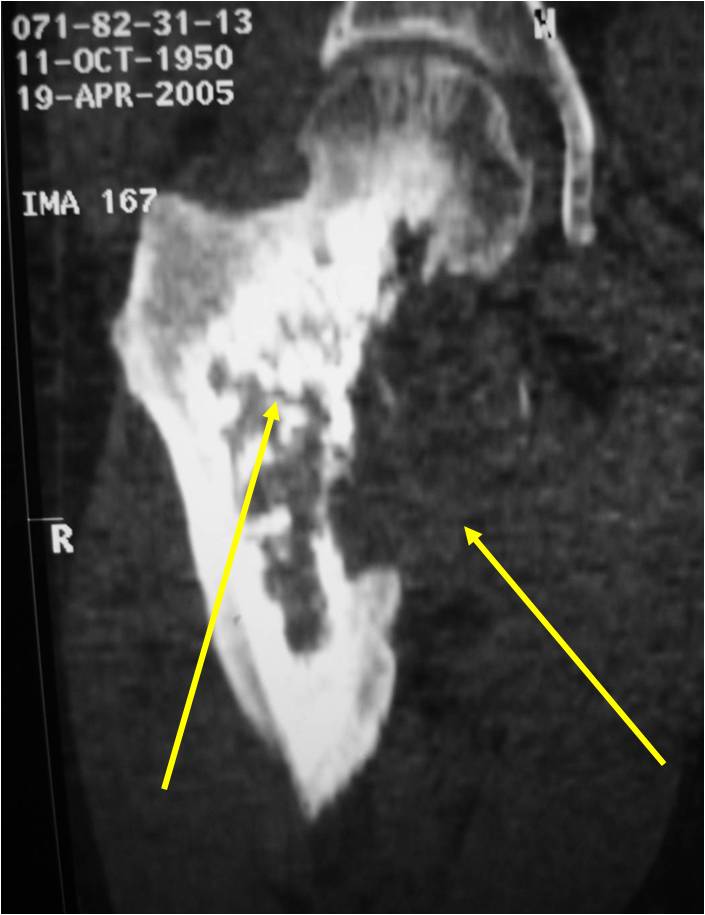
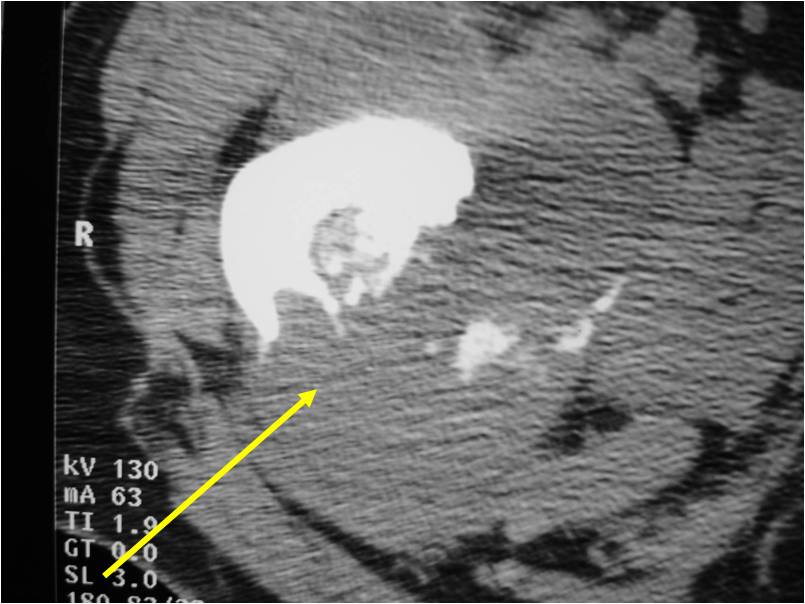
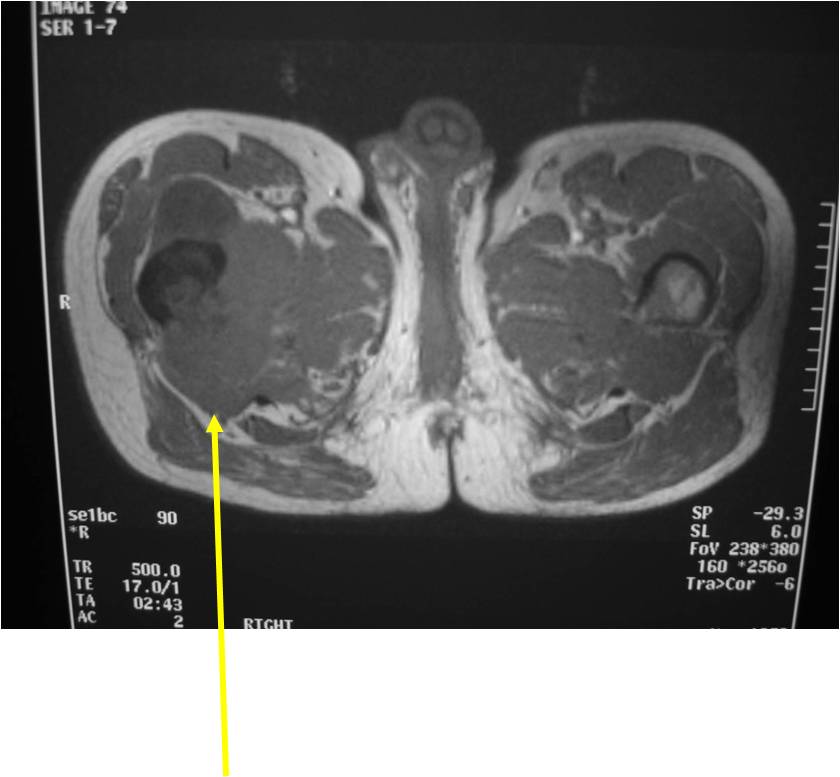
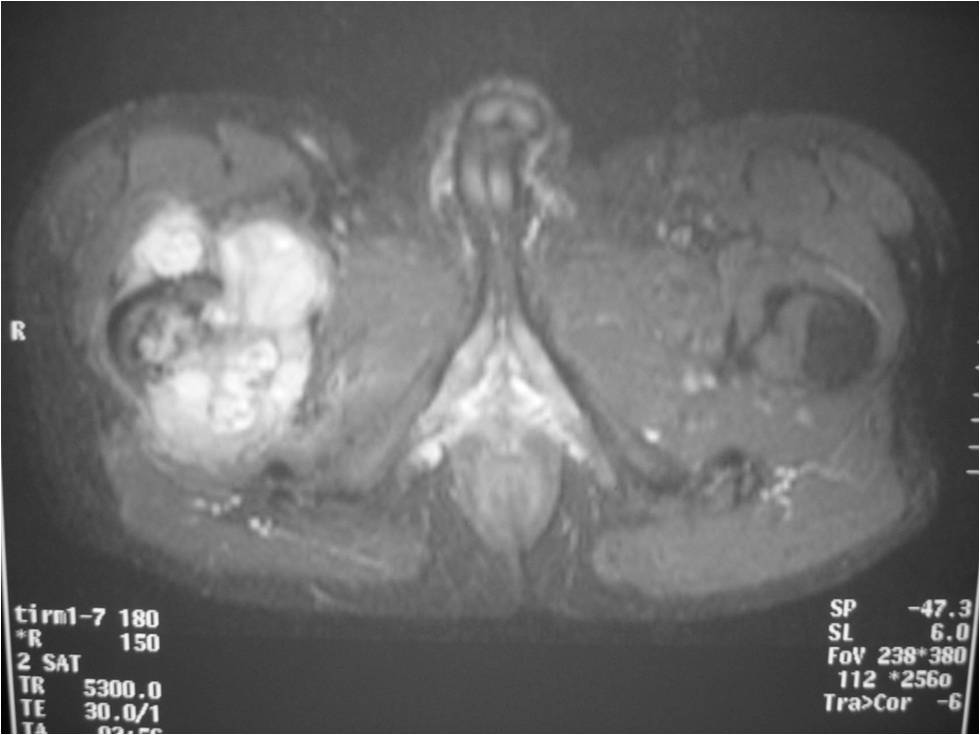
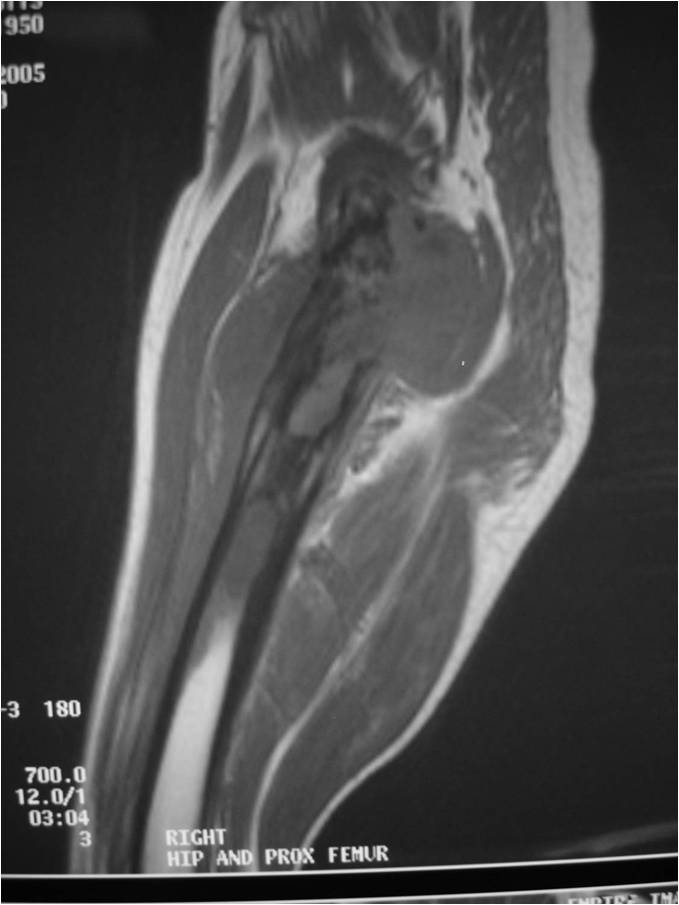
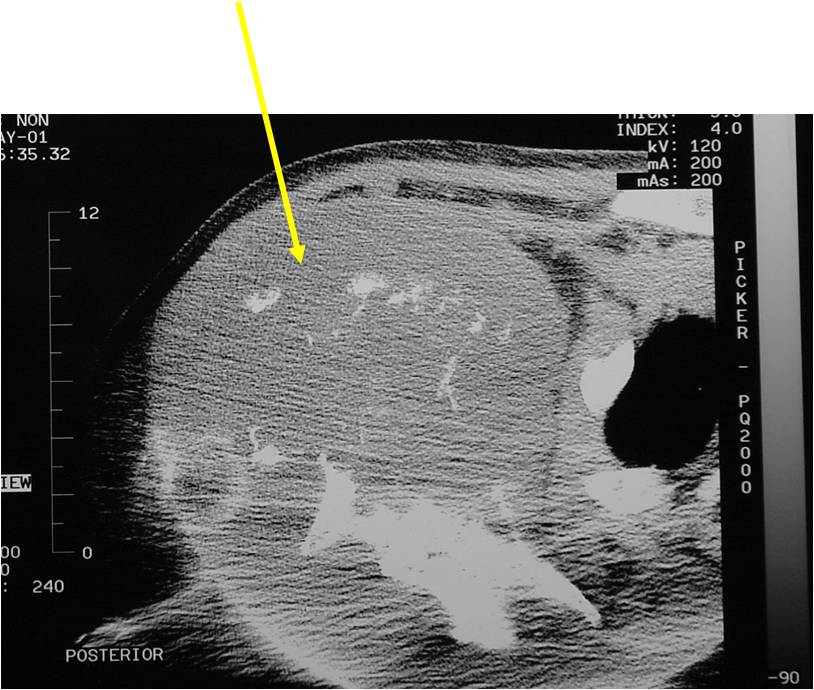
Radiology emulates pathology: Biphasic Tumor
Ill-defined, lytic intraosseous lesion
- Or extraosseous soft tissue mass
- Devoid of calcifications in continuity with lesions having the features of a cartilaginous tumor
Characteristically abrupt transition between chondroid tumor and dedifferentiated, lytic component
Bone may be expanded and adjacent cortex thickened
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
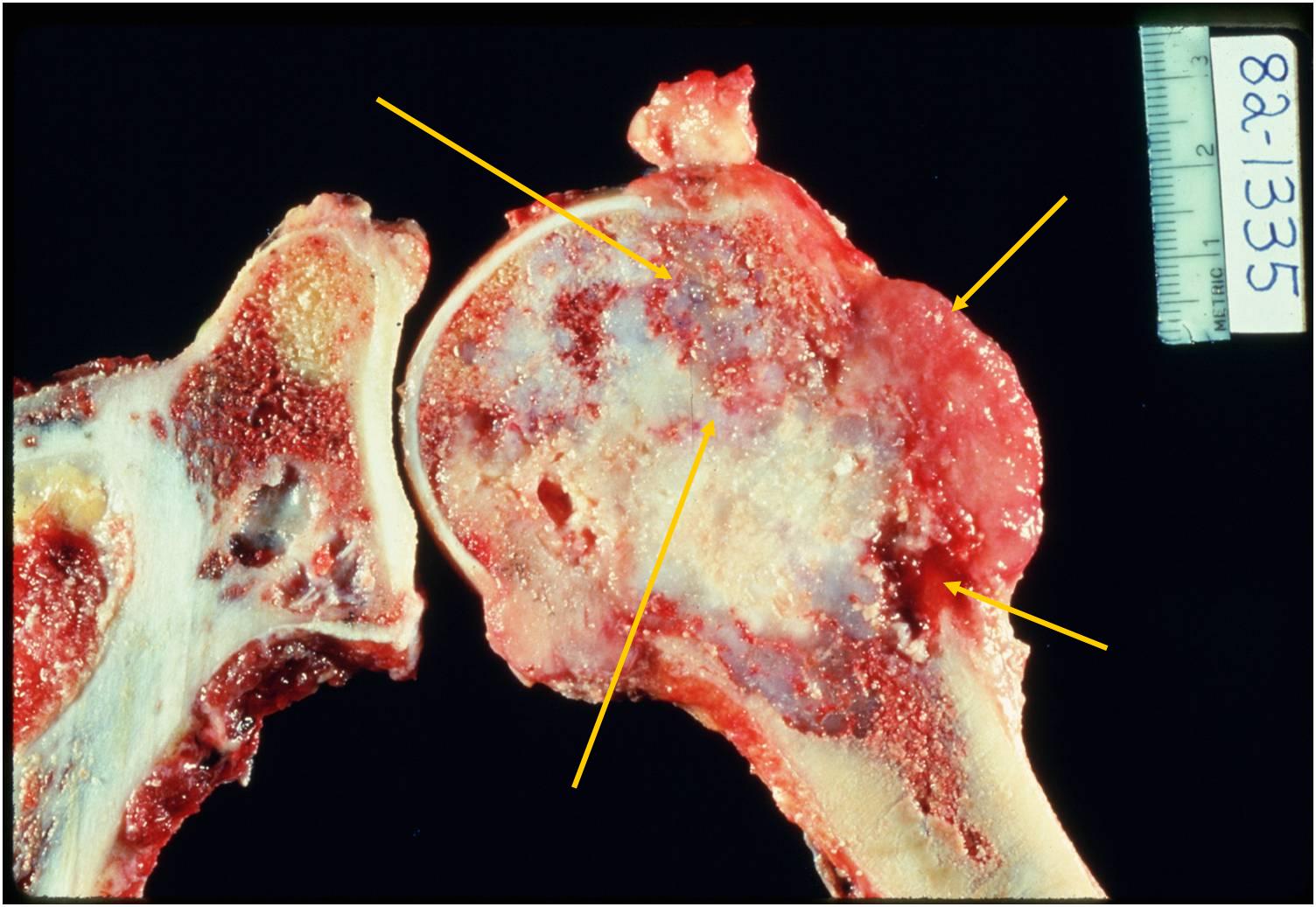
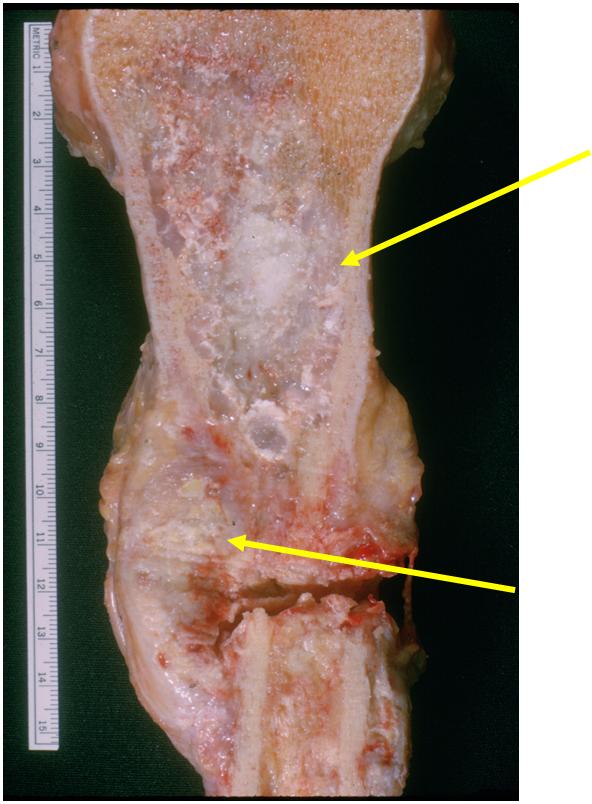
Gross Pathology
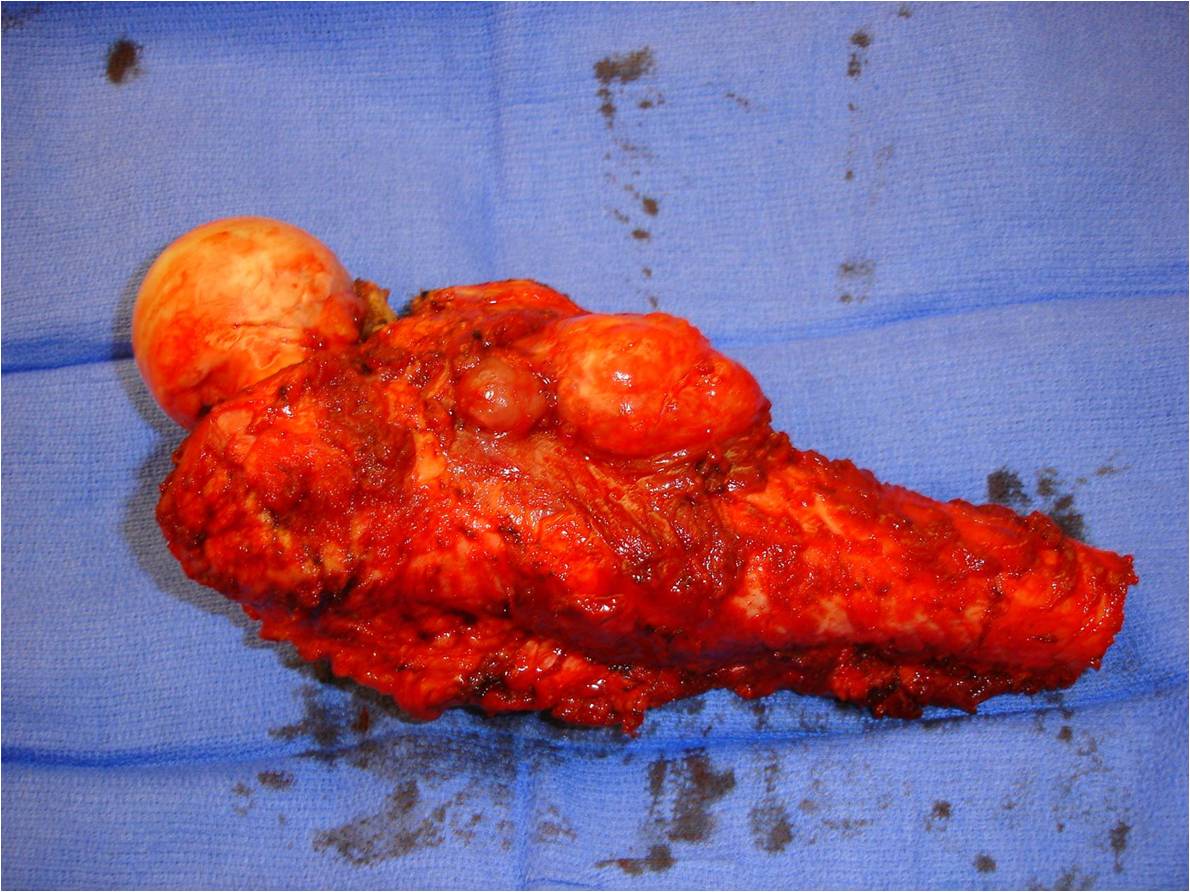
- Areas with typical lobular, blue-gray myxoid hyaline cartilage tissue
- Or overtly cartilaginous appearance of mature hyaline cartilage
- Zones of brown, tan, or hemorrhagic tissue
- Lacking the consistency of cartilage
- Dedifferentiated component may only be a minor portion of the overall tumor
- May also be so extensive that little cartilage is recognizable
| Roll over the images for more information |
 |
 |
 |
 |
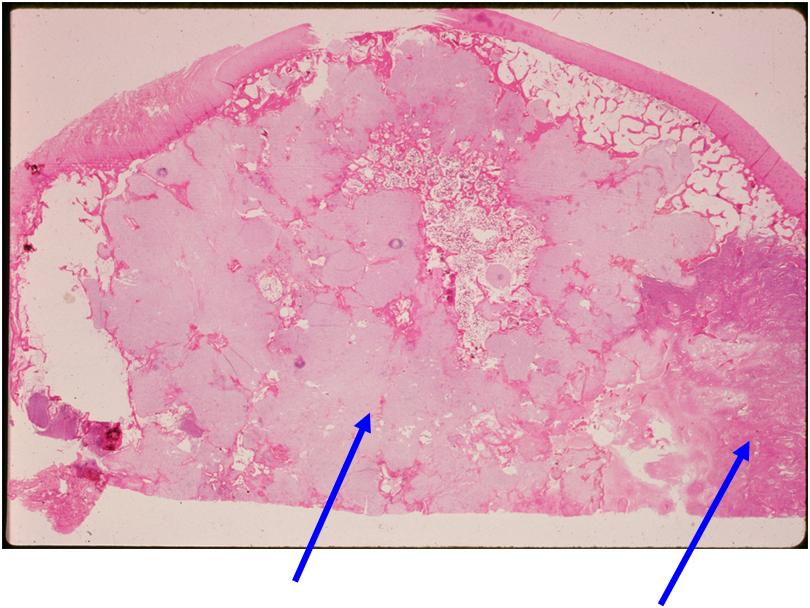
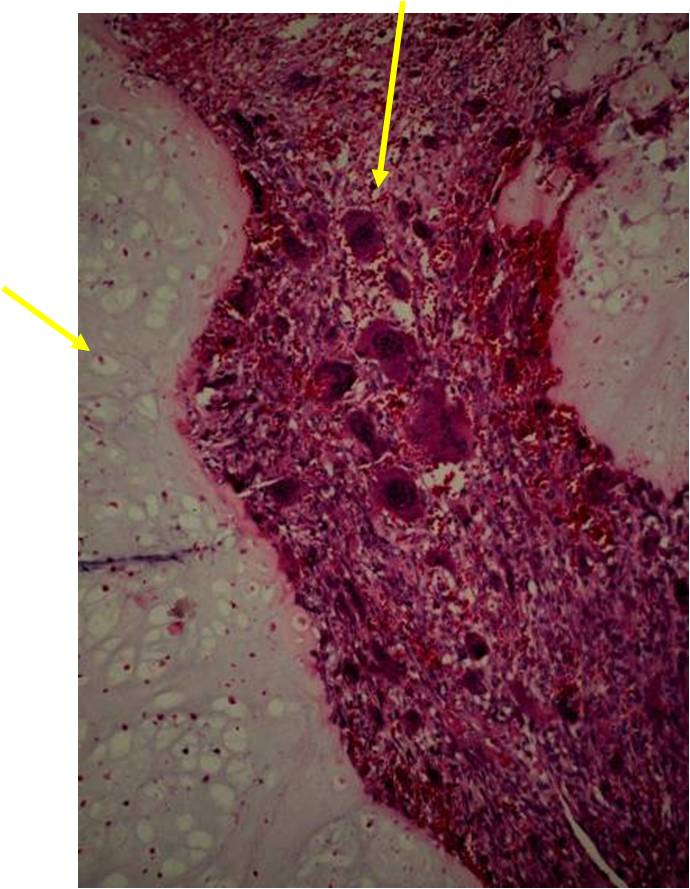
Microscopic Pathology
- Chondrosarcoma component is often grade I (Low Grade Hyaline Type Cartilage)
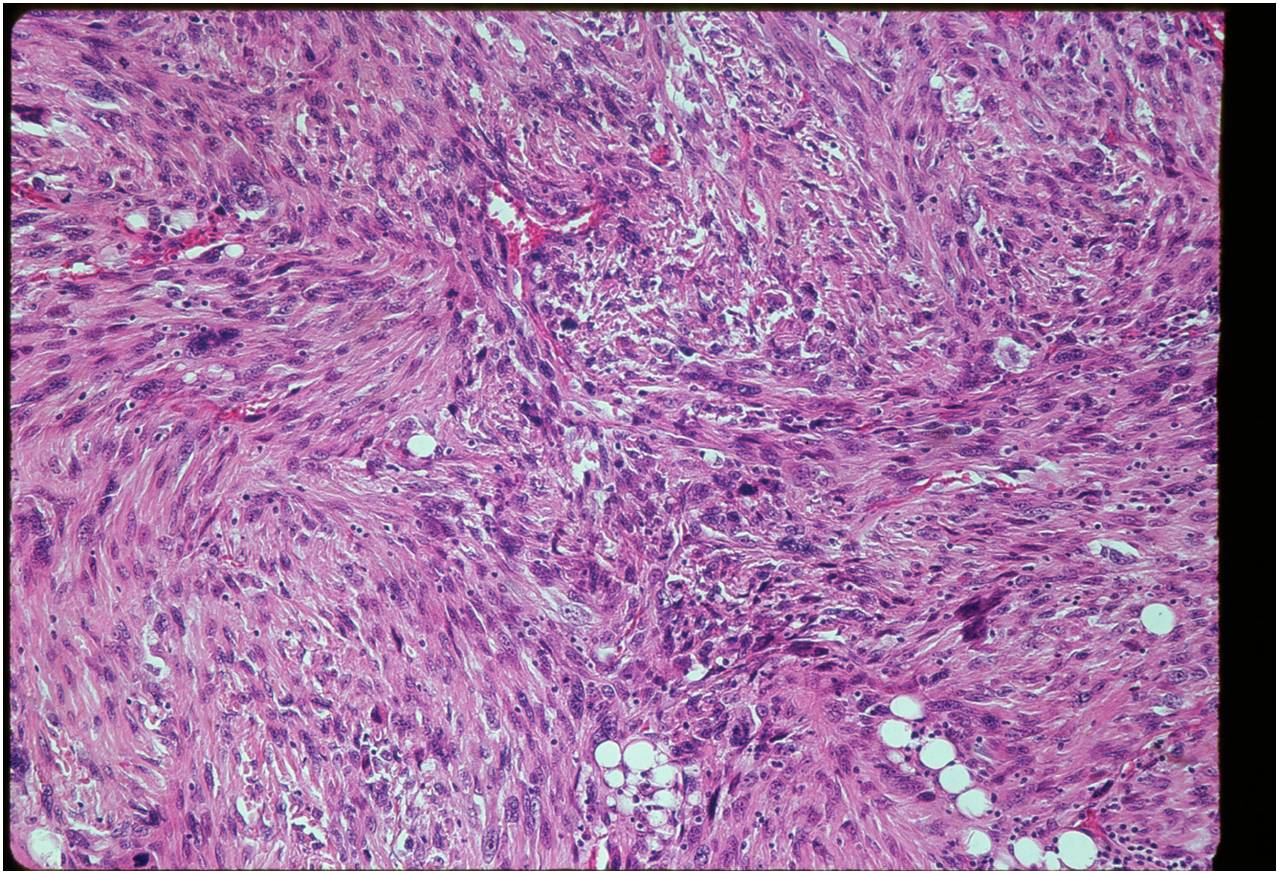
- Dedifferentiated component
- Predominant noncartilaginous/spindle sarcoma component varies
- Fibrosarcoma and MFH most frequently reported
- MFH is a high grade pleomorphic spindle cell tumor with a storiform pattern
- Osteosarcoma is third most common dedifferentiated component
- Rhabdomyosarcoma and angiosarcoma also reported
Junction of cartilaginous and noncartilaginous components is sharp and distinct. There are no dedifferentiated areas admixed in the middle of the cartilaginous areas
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
 |
 |
Differential Diagnosis
- High Grade Chondrosarcoma with Spindle Cell Areas
- Mesenchymal Chondrosarcoma
- Chondroblastic Osteosarcoma
- Malignant Fibrous Histiocytoma
- Fibrosarcoma
Biological Behavior
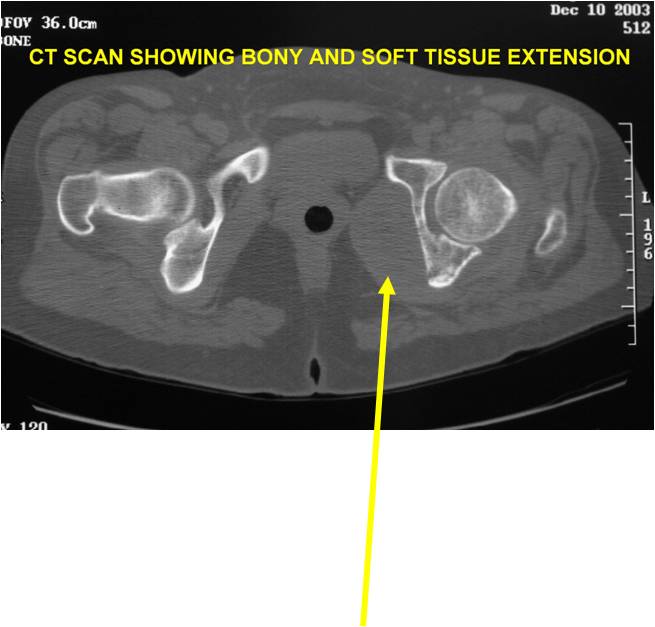
- Very aggressive locally
- Frequently cortical perforation
- Mass is usually large if extraosseous extension occurs
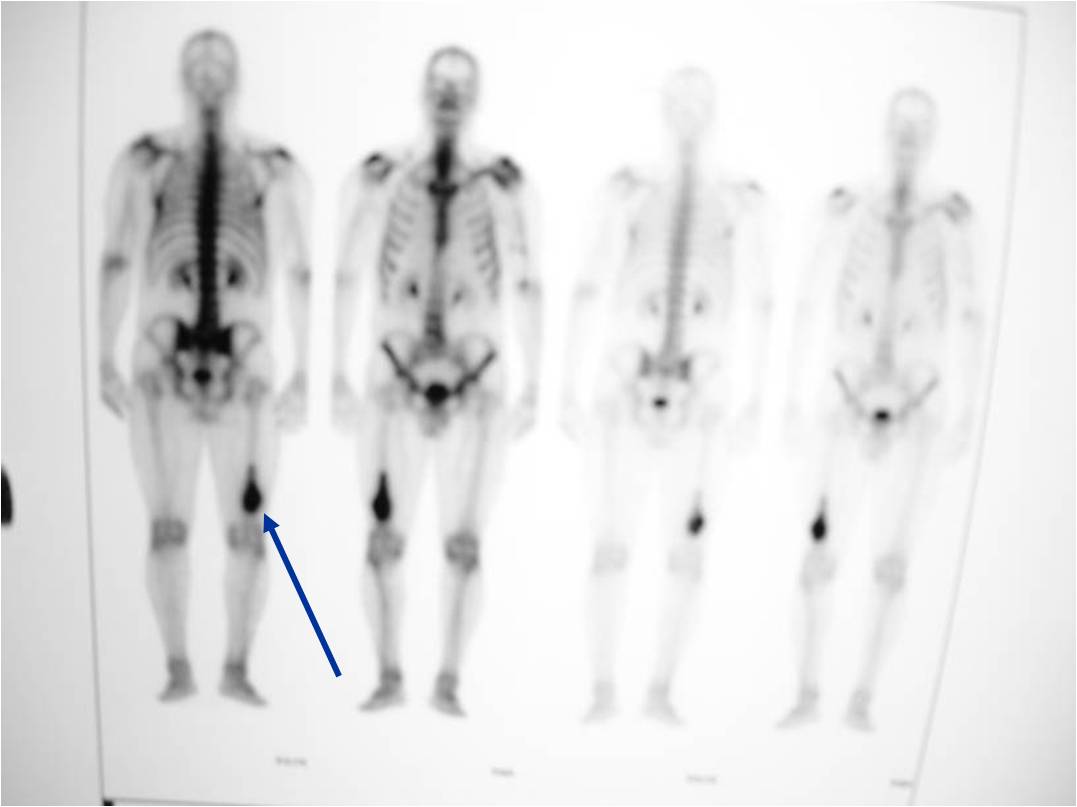
- Extremely high metastatic rate
- Metastasizes primarily to lungs
- Also bones and other organs
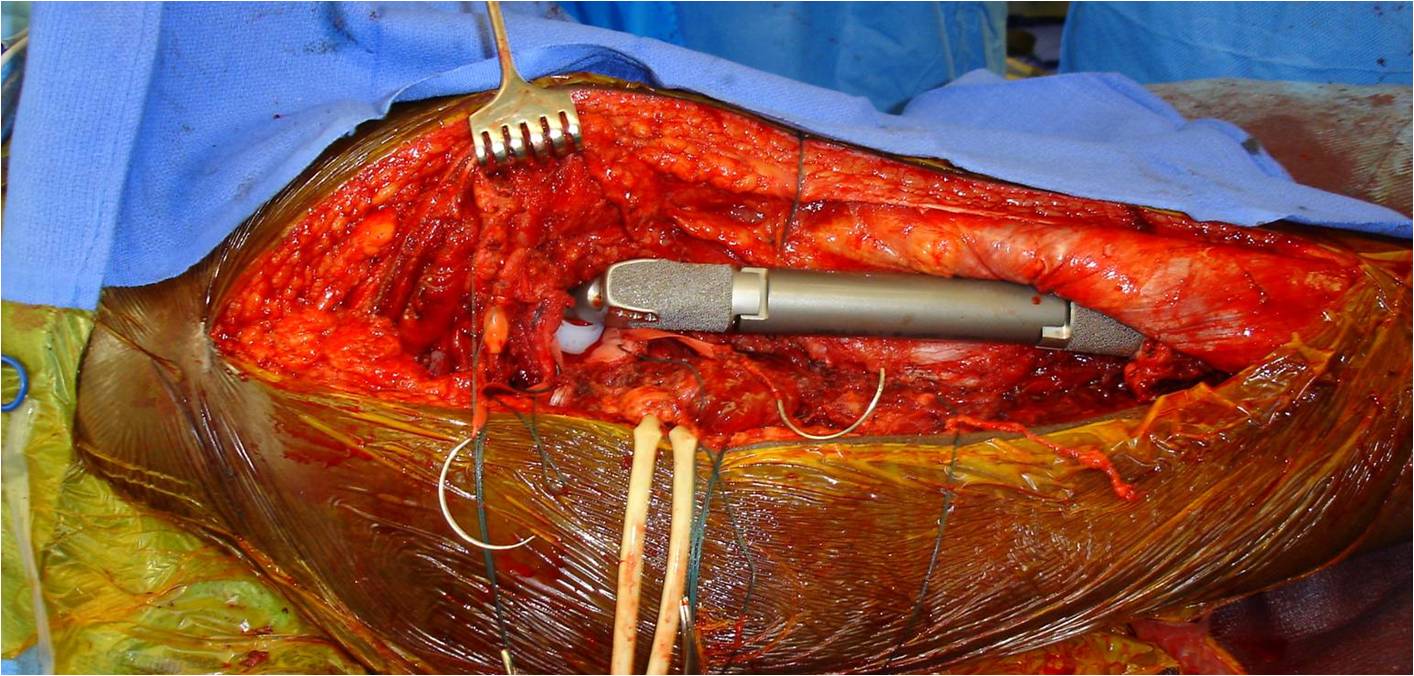
Treatment & Prognosis
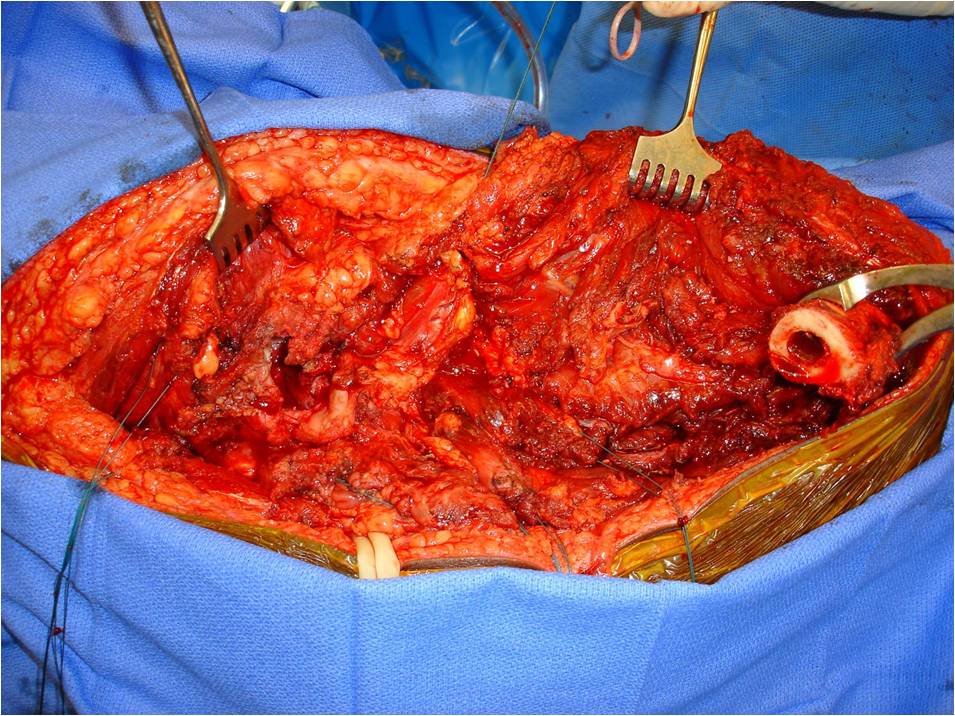
- Wide/Radical limb sparing resection whenever feasible
- Amputation may be necessary for large tumors
- Chemotherapy may be considered for high grade dedifferentiated component but is controversial and no clear cut benefit has ever been demonstrated
- Radiation may be considered if the tumor is unresectable or if a wide margin can not be achieved with surgery such as with large pelvic tumors. Radiation would be used as an adjuvant to eradicate any residual microscopic disease.
- Prognosis almost hopeless, regardless of extent of resection
- 90% of patients are dead of metastatic disease within 2 years
- Most of these die within 1 year
- Metastases consist solely of high-grade dedifferentiated component
- Predominantly in lungs
- Also bones and other organs
| Roll over the images for more information |
 |
 |
 |
 |
 |
