Juxtacortical (Periosteal) Chondrosarcoma
General Information
Juxtacortical/Periosteal
- Similar to juxtacortical chondroma
- Periosteal lesion - cortical erosion
- Chondroid matrix calcification
- Similar to periosteal ogs (no hair on end periosteal reaction)
- Larger soft tissue mass/size (>3-4cm)
- Intramedullary canal spared
Juxtacortical Chondrosarcoma
Definition:
- A malignant, subperiosteal cartilaginous tumor that lacks osteoid production and erodes the underlying cortical bone (periosteal chondrosarcoma)
- <2% of chondrosarcomas
Age:
- 15-63 (80% are >20 years old vs periosteal osteosarcoma and periosteal chondroma)
- No sex predilection
Clinical:
- Painless, mass or swelling; 1/3 of patients have pain (pain rarely exceeds swelling)
- Most Common Locations:
- Femur
- Humerus
- Pelvis
- Rib or foot
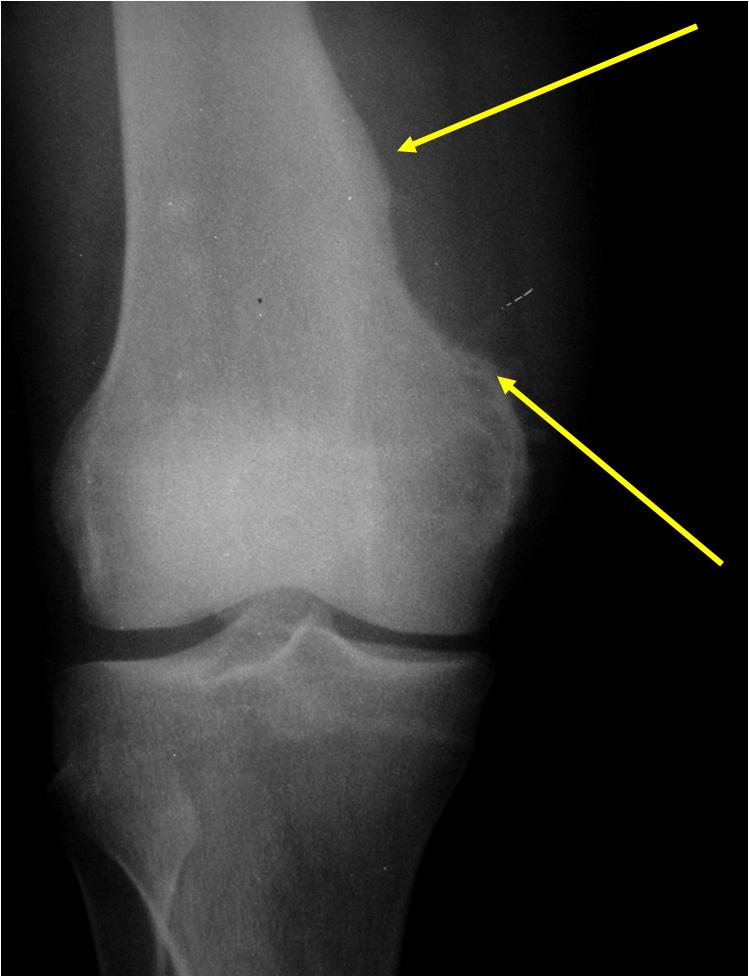
Radiographic Presentation
Radiology:
- Metaphyseal
- Cortical erosion with sclerotic underlying cortex (saucer shaped defect)
- Matrix calcification
- Triangular sclerotic spur at margin of tumor
- >5cm in diameter; average size: 11 cm (vs periosteal chondroma that is usually <5cm)
- No hair on end periosteal reaction (vs. chondroblastic osteosarcoma)
- Intramedullary canal is spared
| Roll over the images for more information |
 |
 |
Differential Diagnosis
- Periosteal Chondroma
- Periosteal Osteosarcoma
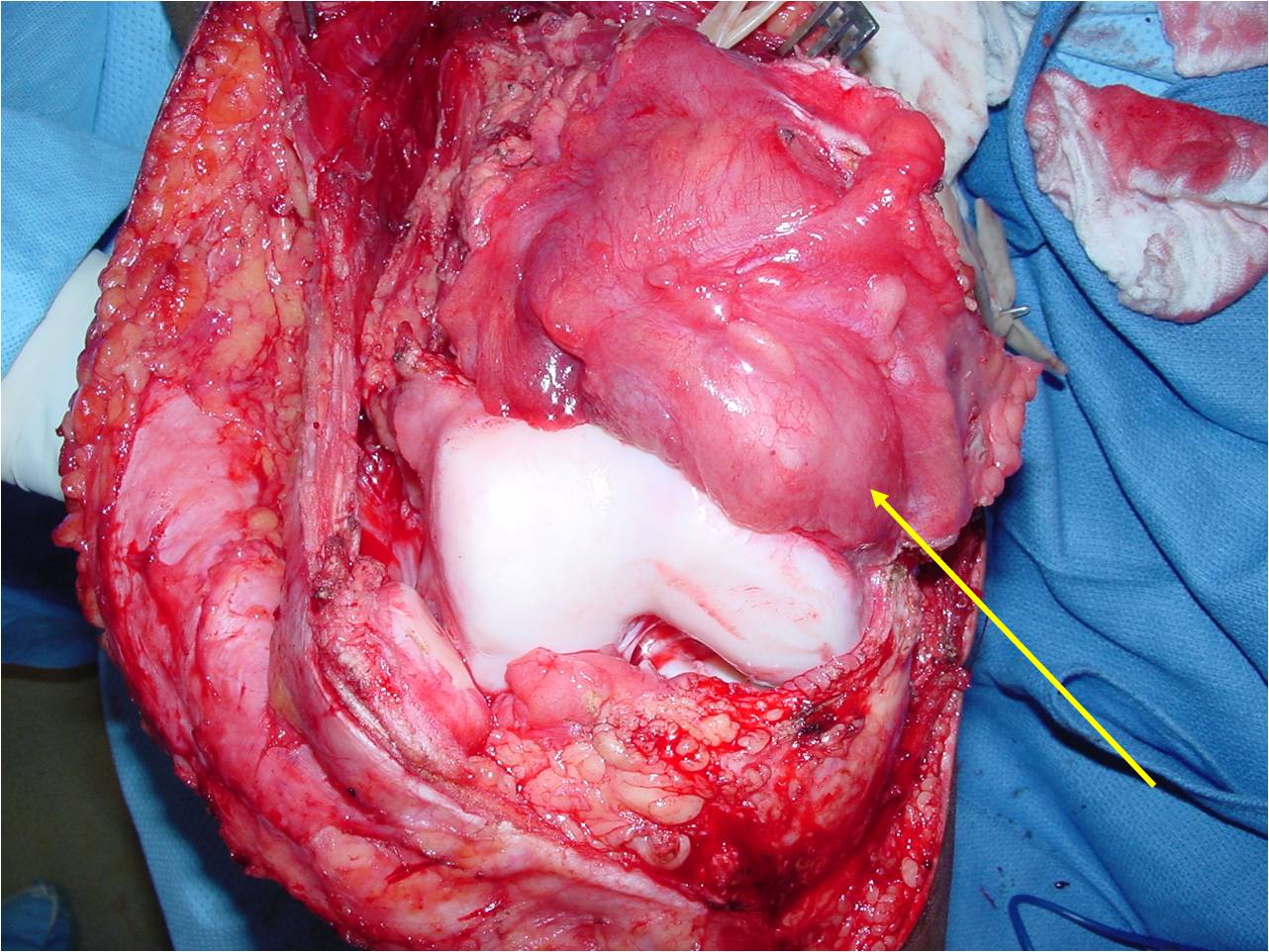
Gross Pathology
- Grossly lobulated, gray-white, translucent
- Calcification is common
- Underlying cortex eroded with irregular sclerotic reaction
Microscopic Pathology
- Lobulated
- Well differentiated, low grade, hyaline cartilage
- Focally myxoid stroma
- No osteoid production
- Almost always grade 1 or 2
- Rarely grade 3
Juxtacortical Chondrosarcoma
Prognosis
- Low rate of Mets
- Metastisizes most commonly to the lungs
- Most are low to intermediate grade tumors
- 80-90% long term survival
Treatment
- Wide Limb Sparing Resection whenever feasible
- Amputation may be indicated for very large, unresectable or recurrent tumors
- Chemotherapy and radiation are generally not used in treatment of periosteal chondrosarcoma
- Chemotherapy may be considered for Grade 3 tumors
- Postoperative radiation may be considered for large tumors that can not be removed with a wide margin
