GENERAL INFORMATION
Low Grade Intraosseous Osteosarcoma is a low grade malignant bone tumor that accounts for 1% to 2% of all Osteosarcomas. Constituent cells of the tumor form osteoid or immature woven bone.
CLINICAL DATA
• More frequent in second and third decades of life.
•
Long bones are the most frequent location (80%)
•
Tumors most commonly arise around the knee
•
Patients commonly present with pain and perhaps an enlarging soft-tissue mass
Differential Diagnosis
• Fibrous dysplasia
• Low-grade fibrosarcomas
• Parosteal osteosarcoma
• Other benign lucent lesions such as osteoblastoma, chondroblastoma, giant cell tumor and non ossifying fibroma depending on location
RADIOGRAPHIC PRESENTATION
Plain x-ray
• Radiographs of low grade intraosseous osteosarcoma may demonstrate a benign appearance (Fig. 1 & 2).
• However, most lesions show intramedullary extension, cortical violation, and soft tissue involvement.
• The majority arise centrally in the bone, from the medullary cavity and more frequently are methaphyseal.
MRI
•
MR Imaging, demonstrates intermediate to hypointense signal on T1-weighted images (Fig. 4 & 5) and hyperintensity on T2-weighted images (Fig. 6 & 7).
• Most cases show an extraosseous mass and cortical disruption on MRI.
• Bone scintigraphy frequently display an increase radiotracer uptake (Fig. 8).

Fig. 1

Fig. 2
Fig. 1 & 2: Plain X Ray of Low Grade Intraosseous Osteosarcoma. AP (Fig. 1) and Lateral (Fig. 2) view of the left knee, shows a mixed sclerotic-lytic lesion in the supracondylar area of the femur. There is no periosteal reaction, cortical destruction, or extraosseous soft tissue mass. The lesion is fairly well circumscribed with a sclerotic margin. The lesion deceptively looks benign
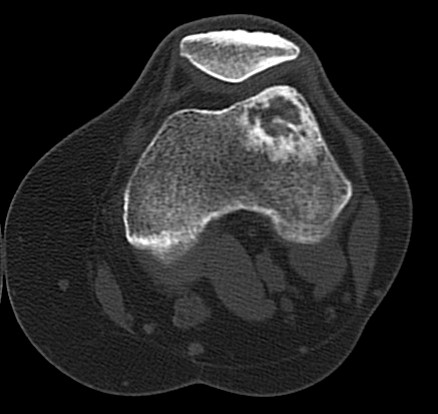
Fig. 3: CT Scan of the left knee showing a lytic lesion within the lateral supracondylar femur with surrounding sclerosis. No definite osseous or cartilaginous matrix was seen.
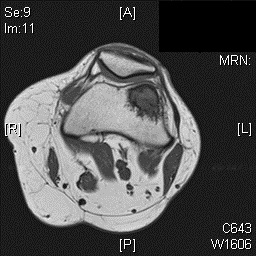
Fig. 4
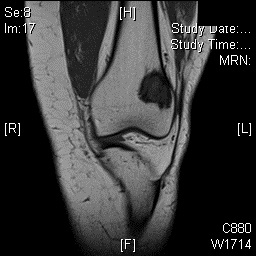
Fig. 5
Fig. 4 & 5: MR Imaging. Axial (Fig. 4) and Coronal (Fig. 5) T1 weighted image demonstrates a well-defined T1 hypointense mass within the femur with a more hypointense border corresponding to the sclerosis noted on the CT
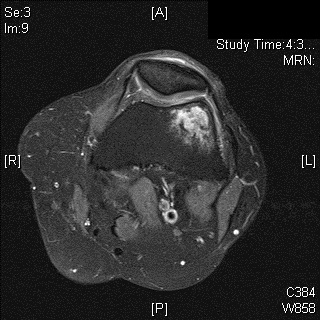
Fig. 6

Fig. 7
Fig. 6 & 7: MR Imaging. Axial (Fig. 6) and Coronal (Fig. 7) T2 fat saturated image demonstrating T2 hyperintense lesion within the lateral supracondylar femur with a small amount of surrounding bone marrow edema.
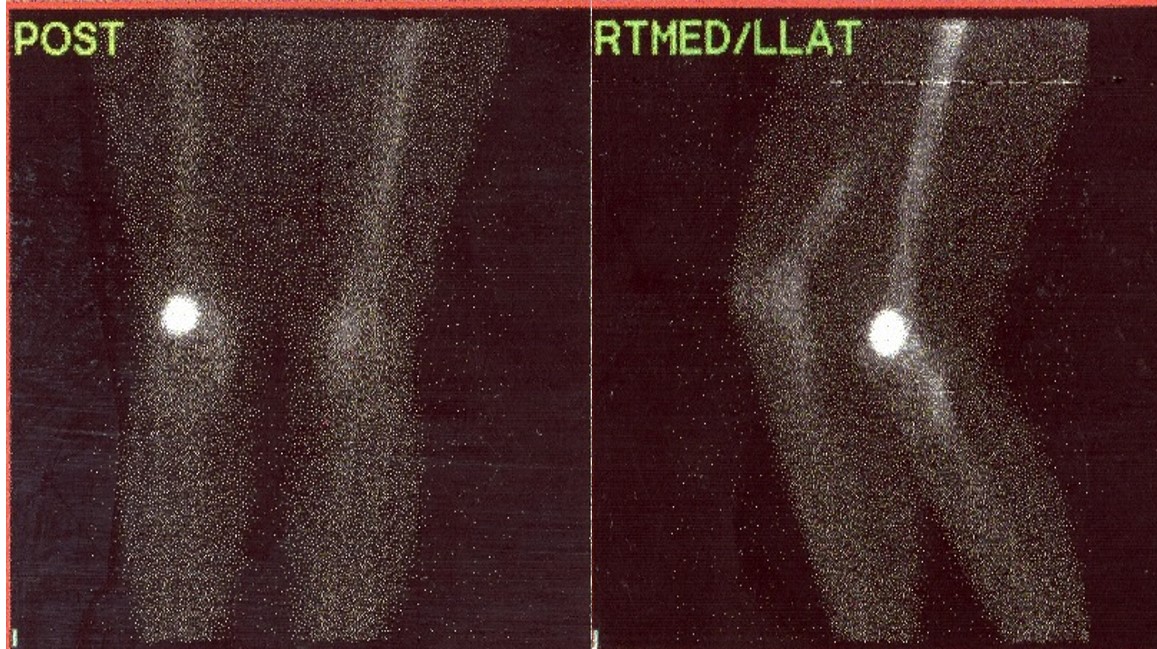
Fig. 8: Bone scintigraphy. Anterior and lateral bone demonstrates increased radiotracer uptake in the left lateral supracondylar femur.
PATHOLOGY
Low Grade Intraosseous Osteosarcoma is a low-grade malignancy, similar to parosteal osteosarcoma.
Microscopic
• D
isplay bundles of spindle cell proliferations with variable osteoid production, low cellularity, low mitotic rate, and minimal pleomorphism (Fig. 9 & 10).
• The presence of infiltrative margins and the absence of marked cellular atypia helps to differentiate low grade intraosseous osteosarcoma from benign entities.
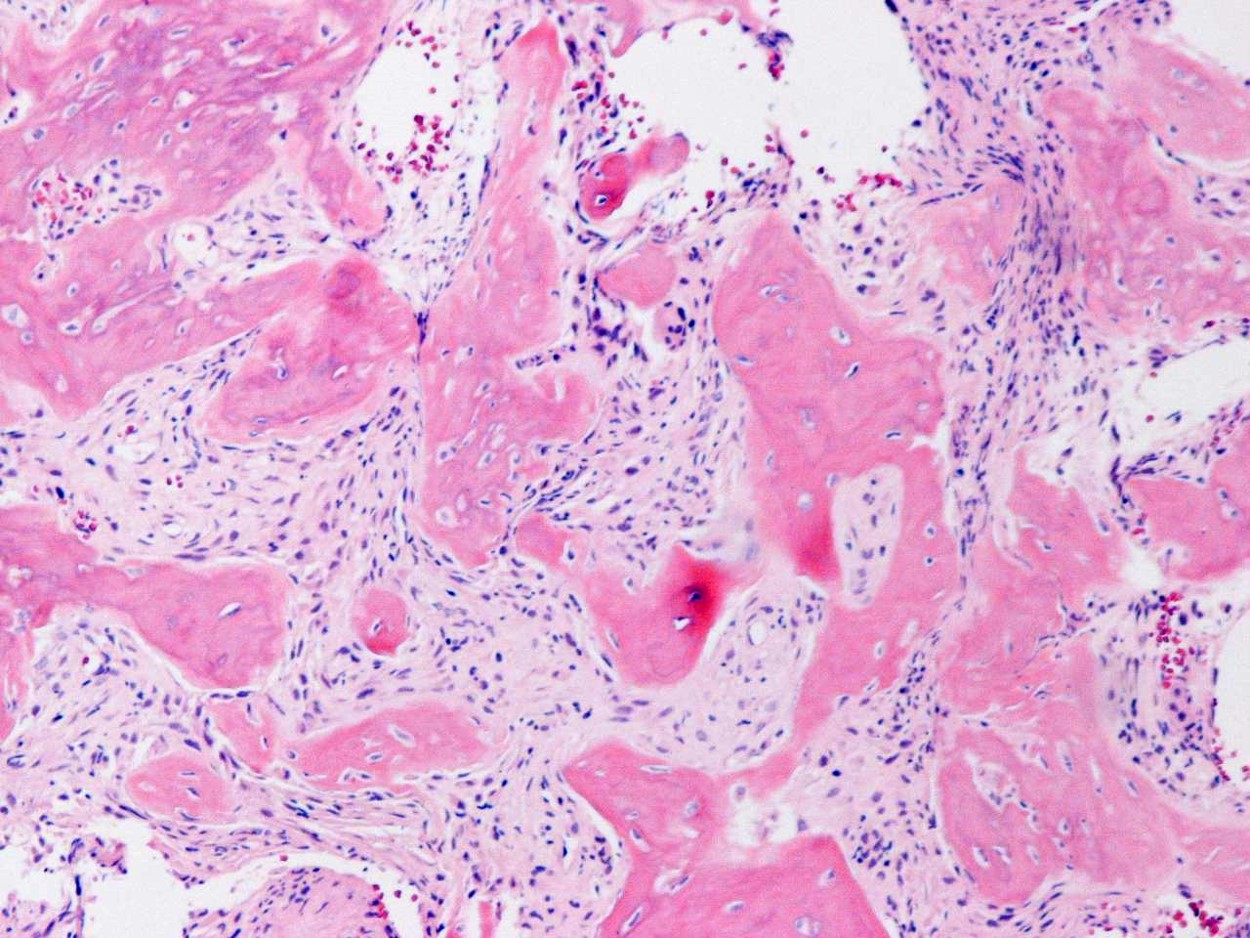
Fig. 9
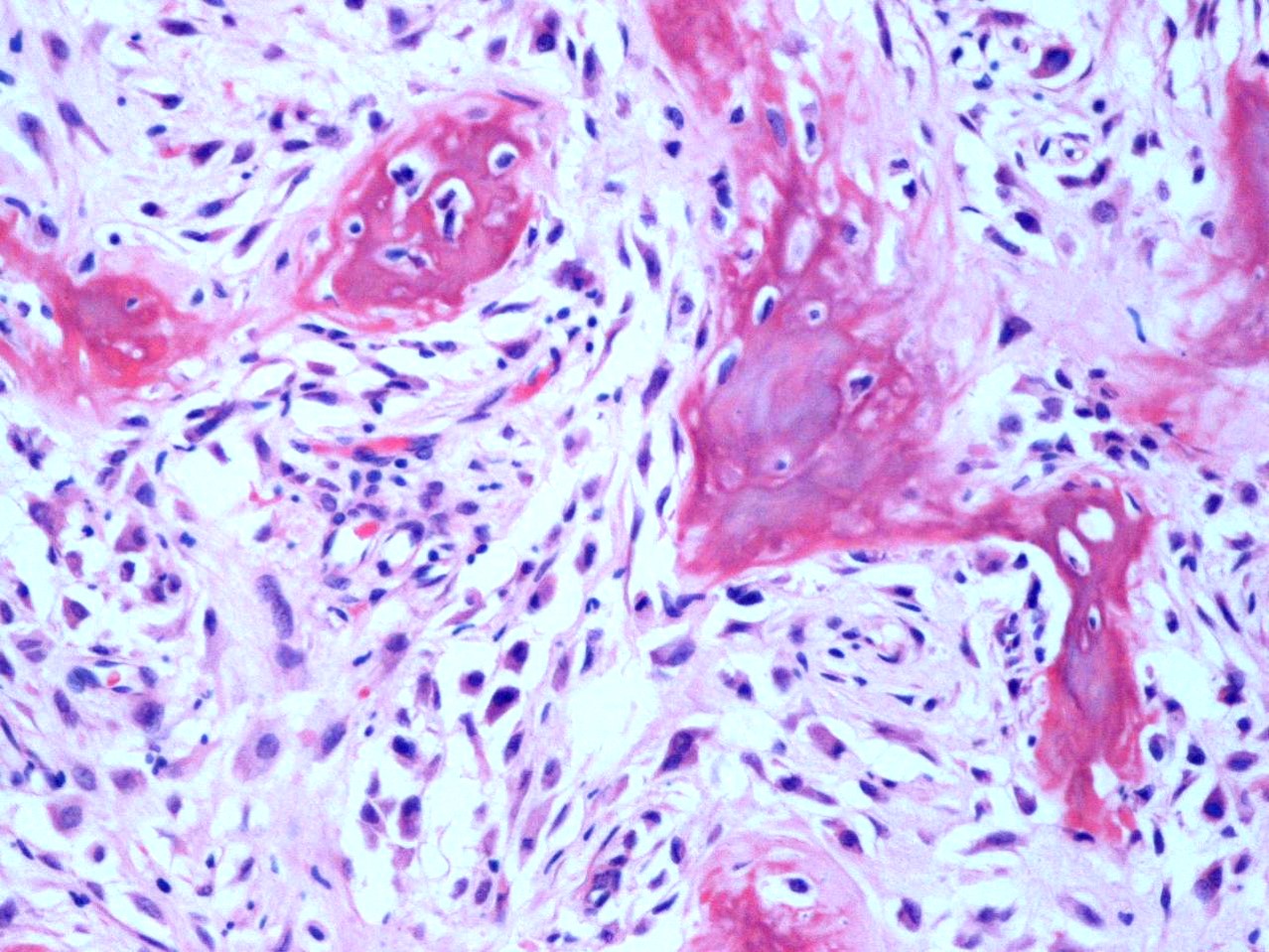
Fig. 10
Fig. 9 & 10: Microscopic Pathology. Low and high power views with irregular woven bone trabeculae in a moderately cellular fibrous tissue. Atypical cells displaying hyperchromatic nuclei are closely associated with the irregular woven bone trabeculae.
TREATMENT
• Treatment is the same for parosteal osteosarcoma.
• Radical / wide resection is the mainstay of treatment.
• Chemotherapy and radiation are usually not indicated as long as the tumor is entirely low grade.
• Rarely, Low grade Intraosseous Osteosarcoma progress to high grade sarcomas.

Fig. 11
