GENERAL INFORMATION
Osteoma is a rare benign bone tumor, composed of mature osseous tissue. It presents as a protruding mass of dense periosteal intramembranous bone, usually on surface of host bone. It is abnormally dense but is normal bone formed in the periosteum. In the extremities they are often an incidental finding.
CLINICAL DATA
• A benign periosteal tumor
•
Rare condition (confused with reactive bone, postraumatic or postinfection, etc)
•
Almost exclusively affect:
• Skull
• Parasal sinus
• Facial bones
•
Multiple osteomas/osteomas involving a long bone, rule out Gardner syndrome (osteomas, colon polyps and desmoid tumors)
Differential diagnosis
• Ossified fibrous dysplasia
• Solid odontomas
• Osteochondromas (in long bones)
• Parosteal osteosarcoma
CLINICAL PRESENTATION
Signs/Symptoms
• Intracraneal osteomas
• Sinus osteomas show signs of nasal and paranasal sinus obstruction
• Extracraneal osteomas
• May cause symptomatic nerve compression
Prevalence
• Sinus osteomas show a male predominance (2:1)
• Maxilla and mandible show female preference (3:1)
Age
• Patients ages range from 10 to 79 years, but most common in the 4th an 5th decades of life
Sites
• Cranium, sinuses and mandible most common
• Long bones-rare
RADIOGRAPHIC PRESENTATION
Plain x-ray
• Sharply defined, radiopaque smooth, homogeneous bone protruding from the surface of a bone
• Almost appears as a localized thickening of the bone
 Fig. 1. AP xray of forearm show a superficial bone lesion in the shaft of the ulna consistent with an osteoma.
Fig. 1. AP xray of forearm show a superficial bone lesion in the shaft of the ulna consistent with an osteoma.

Fig. 2. AP xray of hand show a well circunscribed bone lesion on the 3rd index consistent with a small osteoma.
PATHOLOGY
Gross
•
Most lesions are compact and resemble dense cortical bone
Microscopic
•
Nodules of dense, mature, lamellar bone with orderly arrangement and haversian systems (cortical)
• The bone is very orderly and mature, and organized into lamellae
• The cells are uniform and have small nuclei
• No nuclear pleomorphism and no mitosis
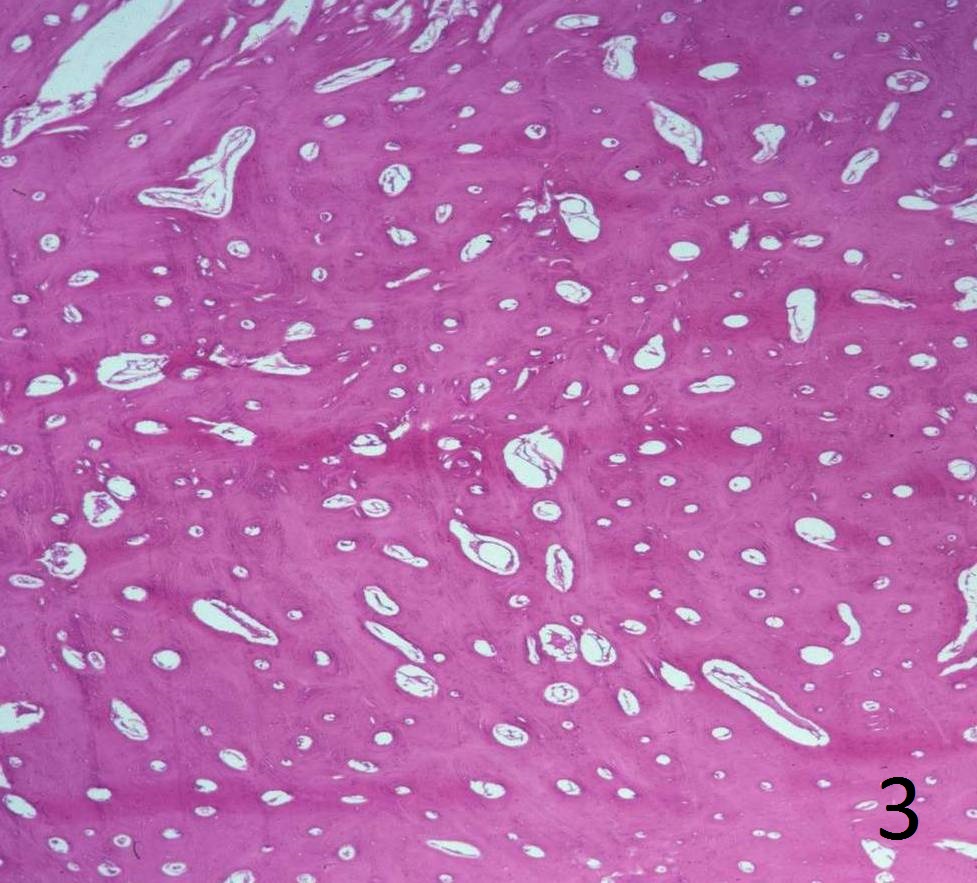
Fig. 3. Low power magnification of lesion, shows a dense thickened lamellar bone with haversian systems.
PROGNOSIS
Biological Behavior
• Sinus lesions may lead to sinusitis or grow into cranial vault
• Recurrence rarely develops
TREATMENT
• Excision vs Observation depending on location and symptoms
• Colonoscopy if Gardner syndrome is suspected
