General Information
- Telangiectatic osteosarcoma is a variant of an intramedullary high grade osteosarcoma.
- Accounts for 3% of osteosarcomas
- Telangiectatic osteosarcoma is extremely lytic on X-rays. It demonstrates very little osteoid production.
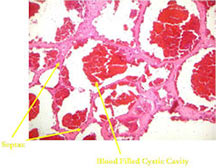
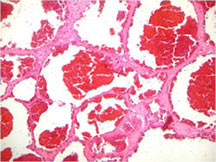
- It is characterized by cystic spaces filled with blood that are separated by thin septa.
- It is a cancerous tumor largely composed of cystic cavities containing necrosis and hemorrhage
- It is postulated that telangiectatic osteosarcomas grow so rapidly that they outgrow there blood supply. Hence portions of the tumor die (undergo necrosis) and form cystic cavities that fill with hemorrhage.
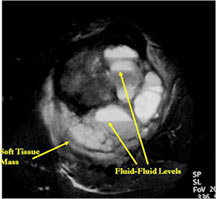
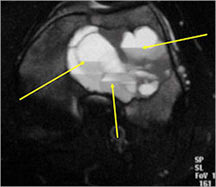
- The cystic spaces filled with hemorrhagic material leads to the presence of fluid-fluid levels on MRIs (so called ABC-like changes or telangiectatic change)
- ABC- like changes can sometimes lead to a misdiagnosis on X-rays and the tumor may be misinterpreted as being a benign ABC.
Clinical Presentation
Signs/Symptoms:
- Similar to Conventional Osteosarcoma
- Dull pain and swelling for a few months duration are common presenting symptoms
- Night pain
- Alkaline phosphatase levels are usually normal
- Pathologic fractures occur in 25% of patients because the lesion is extremely lytic.
Sex:
Age:
- Affects most patients in the second decade of life (teenagers)
- Sites: 50% of cases located in knee area
- Distal femur, proximal humerus, proximal tibia
- Most arise from the metaphysis (90%); diaphyseal (10%)
Radiology
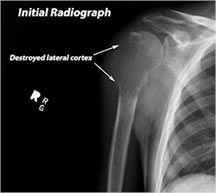
X-ray:
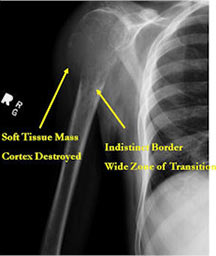
- Permeative lesion with indistinct border that is poorly marginated
- Osteolytic and expansile on X-ray with very little osteoid production
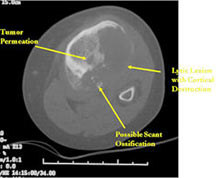
- Osteoid usually not discernible on X-ray but scant and faint lace-like osteoid may be detectable on a CT scan
- No surrounding sclerosis
- May have Codman's triangle and malignant appearing periosteal reaction in most cases
- Cortical destruction and soft tissue extension are common
- Pathologic fracture (25%-30%)
- Expands contour of bone and may appear similar to an ABC (aneurysmal bone cyst)
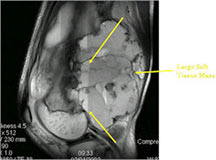
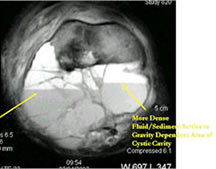
MRI/CT:
- Fluid-fluid levels secondary to cystic cavities filled with blood products. The sediment from blood products settle to the gravity dependent area of the cavity and the fluid component floats to top thus forming a fluid-fluid level.
- MRI and CT are also useful for demonstrating the local extent of the tumor and any soft tissue mass
- CT also useful for demonstrating scant osteoid production
Bone scan:
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
|
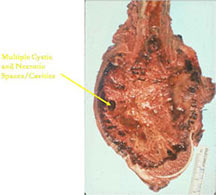
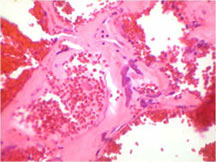
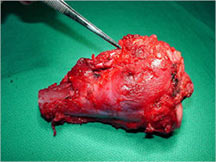
Pathology
- Telangiectatic osteosarcomas have a variable gross appearance
- They may appear as a large blood clot filling a single large cystic cavity; hemorrhagic and necrotic mass; or a multicystic fluid-filled lesion
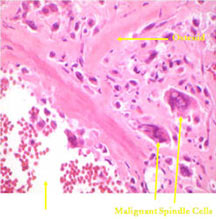
- Thin septae exist between the cystic cavities that harbor malignant appearing spindle cells producing scant osteoid
- Fleshy and sclerotic tissue typical of a conventional osteosarcoma is not seen
- Its gross appearance can mimic an aneurysmal bone cyst
- Mixture of large cystic and spongy areas
| Roll over the images for more information |
 |
 |
 |
 |
 |
|
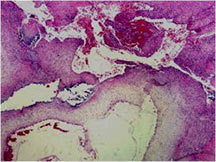
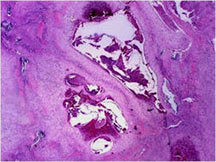
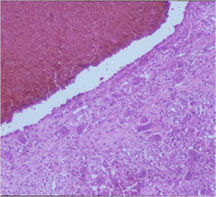
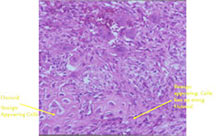
Microscopic Pathology
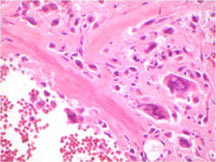
- Tumor has cyst-like spaces divided by septa
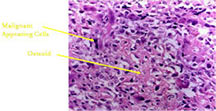
- Septa composed of atypical, bizarre, malignant appearing spindle cells with atypical nuclei and atypical mitotic figures
- Osteoid production is scant, focal and lace-like
- High degree of nuclear atypia, cellular pleomorphism, normal and atypical mitotic activity
- In highly necrotic tumors that appear grossly as blood clot, malignant cells may be separated in a background of necrotic and bloody debris and may be difficult to identify.
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
 |
 |
 |
|
Differential Diagnosis
Conventional osteosarcoma with dilated vascular spaces
Aneurysmal Bone Cyst (ABC)
- ABC usually has more sharply defined margins
- ABC usually has peripheral “egg shell†calcification indicating that the periosteum is intact around the soft tissue component (a benign radiographic feature)
- ABC may have osteoid production in wall but the osteoid is usually surrounded by benign appearing osteoblasts with plump cytoplasm and uniform features; the osteoid is typically laid down in a sheet or trabecular appearance
- Telangiectatic osteosarcoma has bizarre, atypical malignant cells and scant, lace-like osteoid
| Roll over the images for more information |
 |
 |
 |
|
Biological Behavior
- Fast growing, rapidly dividing, high grade tumor with high risk for metastases (spreading)
- With tumor progression
- Massive bone destruction
- Formation of large palpable soft tissue mass
- Often invasive growth of surrounding soft tissue with cortical erosion
- Metastases (similar to conventional osteosarcoma):
- Lungs are most common sites of metastases
- Bones are second most common site
Treatment/Surgery
- Preoperative (induction) chemotherapy (typical regimens utilize these medications; treatment usually follows same regimen as conventional osteosarcoma; most patients are treated according to Children’s Oncology Group Protocols):
- Adriamycin (doxorubicin)
- Cisplatinum (cisplatin)
- High Dose Methotrexate (HDMTX)
- Ifosfamide/Etoposide in some regimens
- (usually 2 or 3 cycles and then surgery)
Surgery:
- Wide surgical resection/limb salvage
- Amputation for large unresectable tumors and other rare instances
Postoperative (adjuvant) chemotherapy:
- Same regimen as preop; usually 4 cycles but can vary
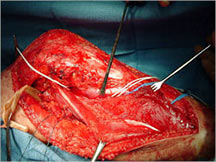
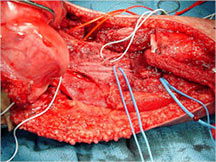
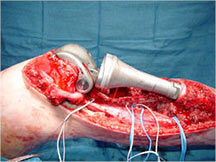
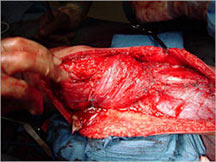
Limb Sparing Surgery
- Surgical principles are the same as those employed for conventional osteosarcoma
- Nowadays, most patients can be treated with a limb sparing resection instead of an amputation
- Prosthetic replacements, cadaver allografts, vascularized bone grafts as well as other methods have been used to reconstruct extremities after tumors are removed
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
Prognosis
Telangiectatic osteosarcoma has a similar prognosis as conventional osteosarcoma
Overall 5-year survival rate depends on site, size, resectability, presence of metastasis
- There is approximately an overall 65% 5 year survival rate for patients who present without overt metastases
- Patients who respond well to preoperative chemotherapy have a better prognosis than those who have a poor response
- Patients who present with or develop metastases have a worse prognosis
