General Information
Codman Tumor (old historical name for chondroblastoma)
- Cartilage Containing Giant Cell Tumor (Kolodney 1972)
- Calcifying Giant Cell Tumor (Ewing 1928)
Clinical Data
- Rare; 1-2% all bone tumors
- Male predilection (2:1)
- Children and young adults; 90% 5-25 yrs. old
Benign aggresive tumor with high propensity for local recurrence
Very rare cases that metastasize to lungs
Location: almost all cases arise from epiphysis of bone
- Epiphysis/apophysis only 40% of cases
- Epiphysis and metaphysis 55% of cases
- Metaphysis only 4%
Differential diagnosis of epiphyseal lesions
- Chondroblastoma
- Clear cell chondrosarcoma
- Giant Cell Tumor (GCT)
- Subchondral Cyst/Intraosseous Ganglion
- Infection
- Eosinophilic Granuloma (LCH)
- Osteoid Osteoma
- Osteoblastoma
- Mets, myeloma, lymphoma
Clinical Presentation
Signs/Symptoms:
- Mild Pain lasting from months to several years
- 33% of patients have a joint effusion and swelling with limitations in range of motion
- Often confused with a sports injury
Prevalence:
Age:
- Range 3-72 years
- 95% of cases occur between the ages 5 and 25
- Most cases occur in adolescents between 10 and 20 years of age
Sites:
- Predilection for distal femur, proximal tibia & humerus
- 98% located in epiphysis, 30% in knee area
- May also occur in calcaneus, talus and temporal bone
Most common locations:
- Proximal Femur 23%
- Distal Femur 20%
- Head and Neck 16%
- Trochanter 7%
- Proximal Tibia 17%
- Proximal Humerus 17%
- Hands and Feet 10%
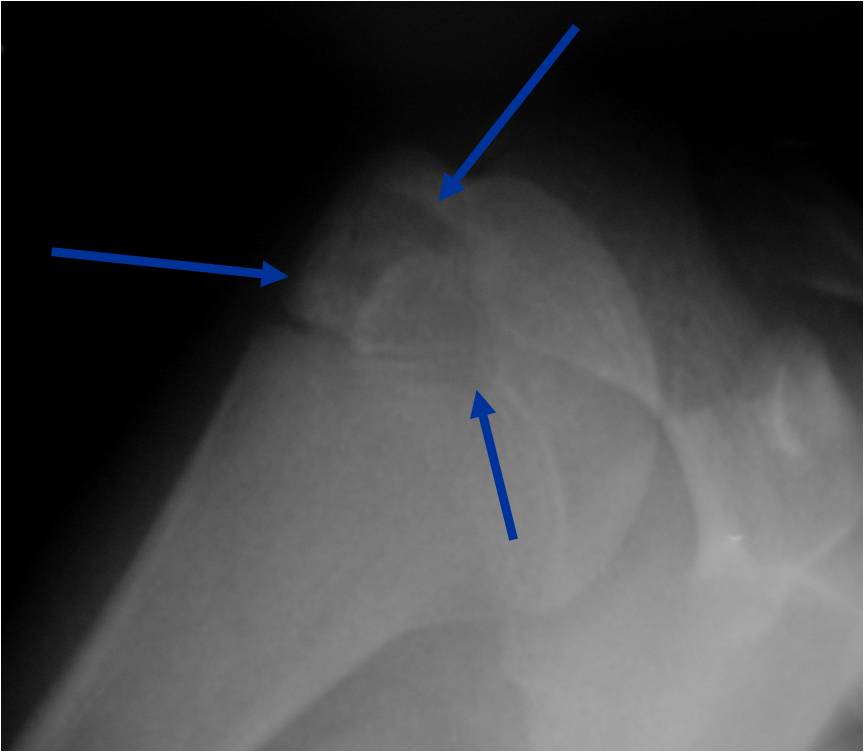
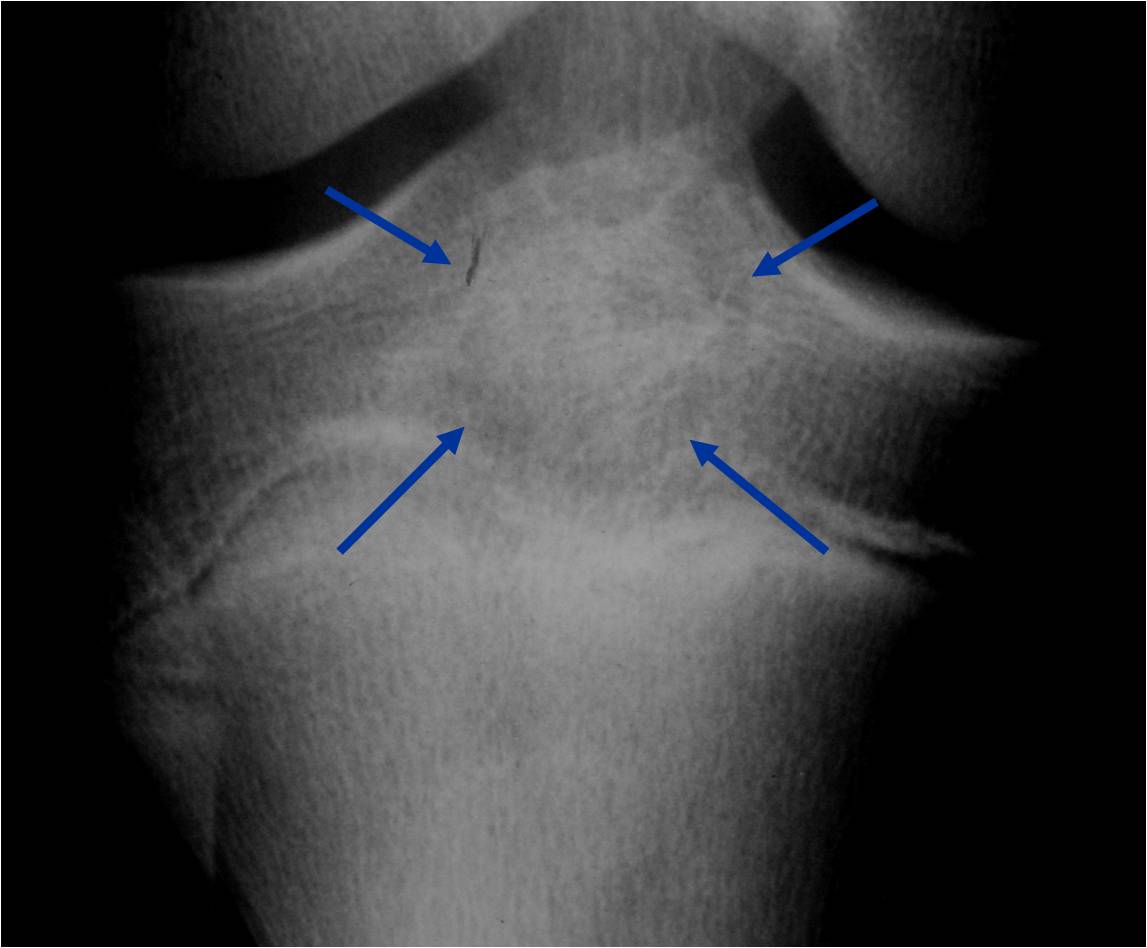
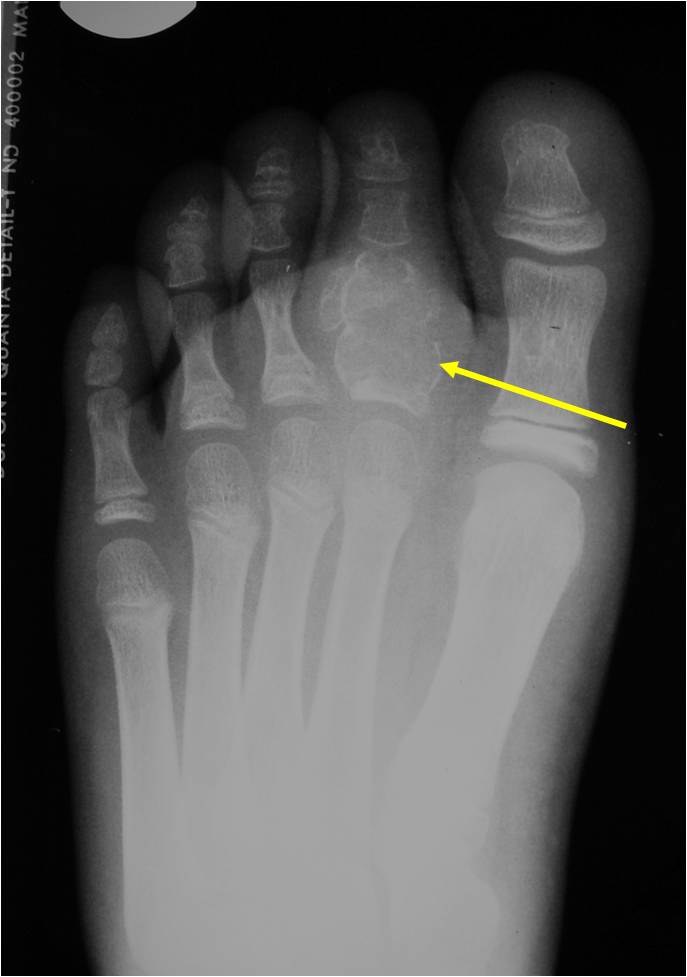
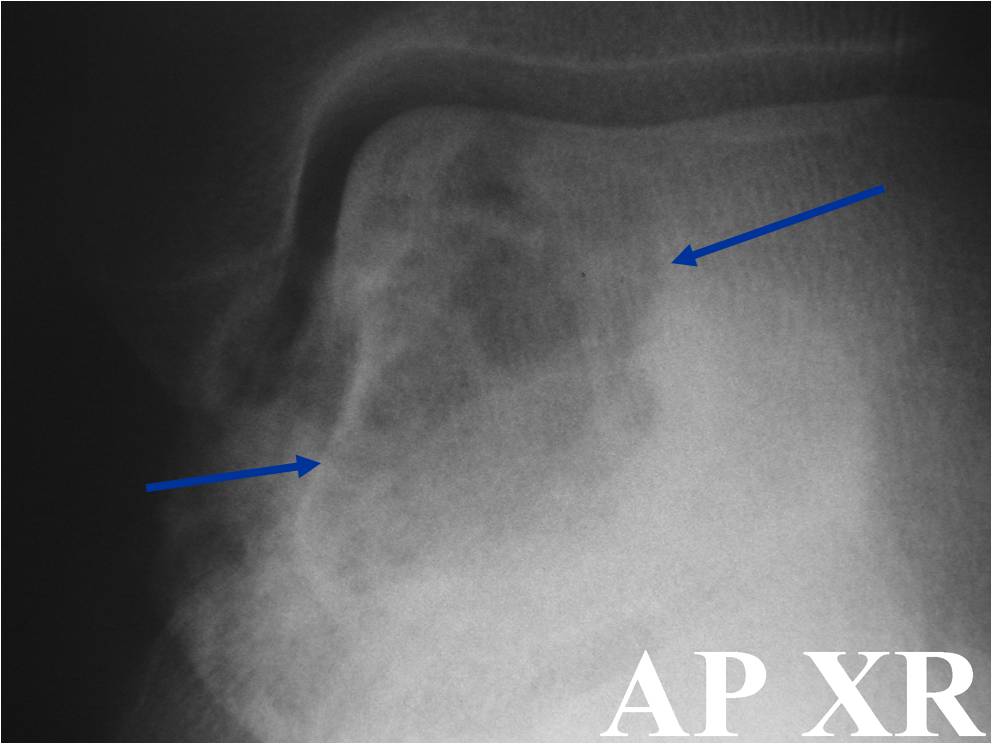
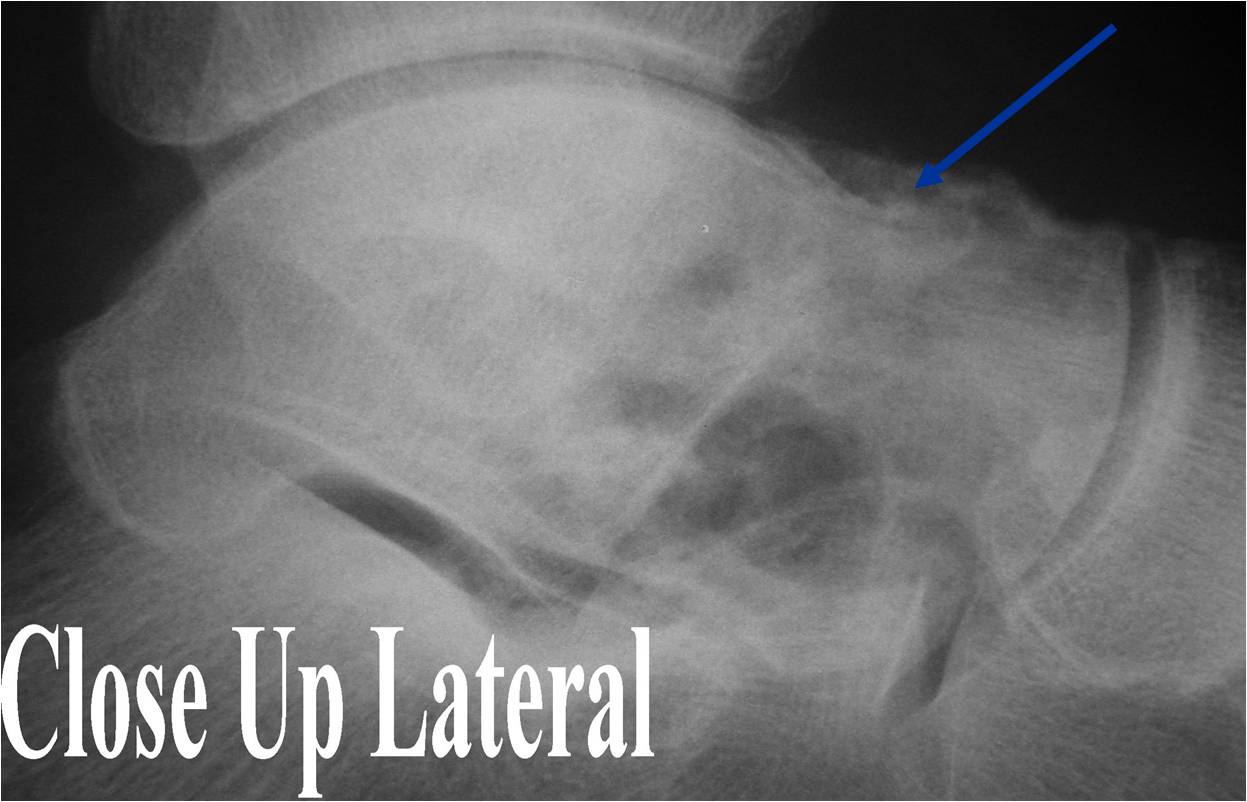
Radiographic Presentation
- Presents as a highly defined/well circumscribed geographic oval/round lytic defect
- Surrounded by rim of sclerotic bone
- Usually in epiphyseal region
- Lesion ranges from 3 cm to 6 cm diameter
- Usually radiolucent
- May have fine trabeculae and irregular calcifications
- Calcifications are often better detected with a CT scan but are not uniformly present
- Lesions may expand the bone and new periosteal bone may form
- Bony end plate, cortex, bone contour are unaffected
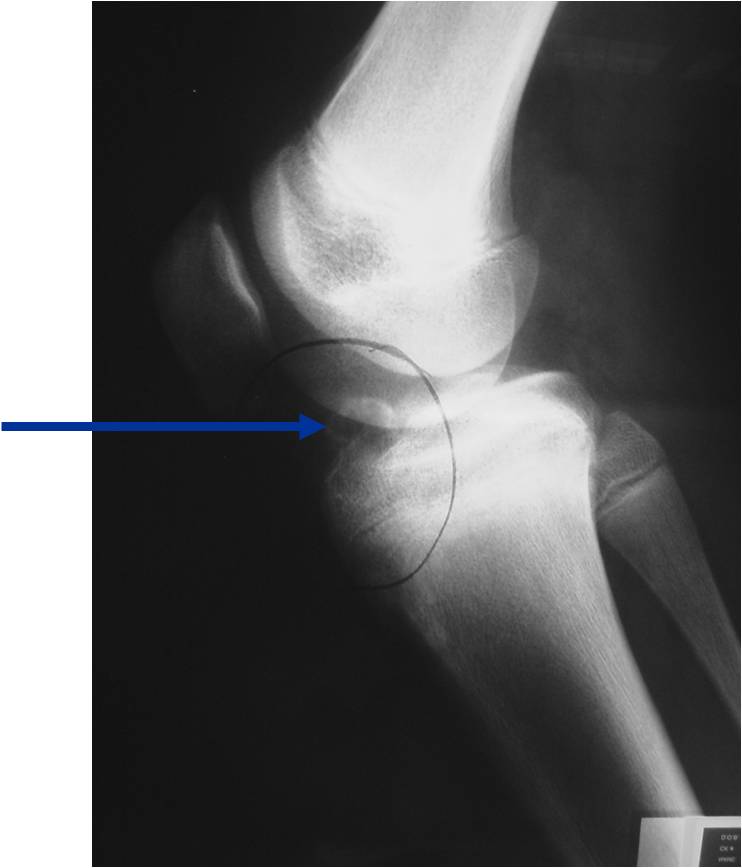
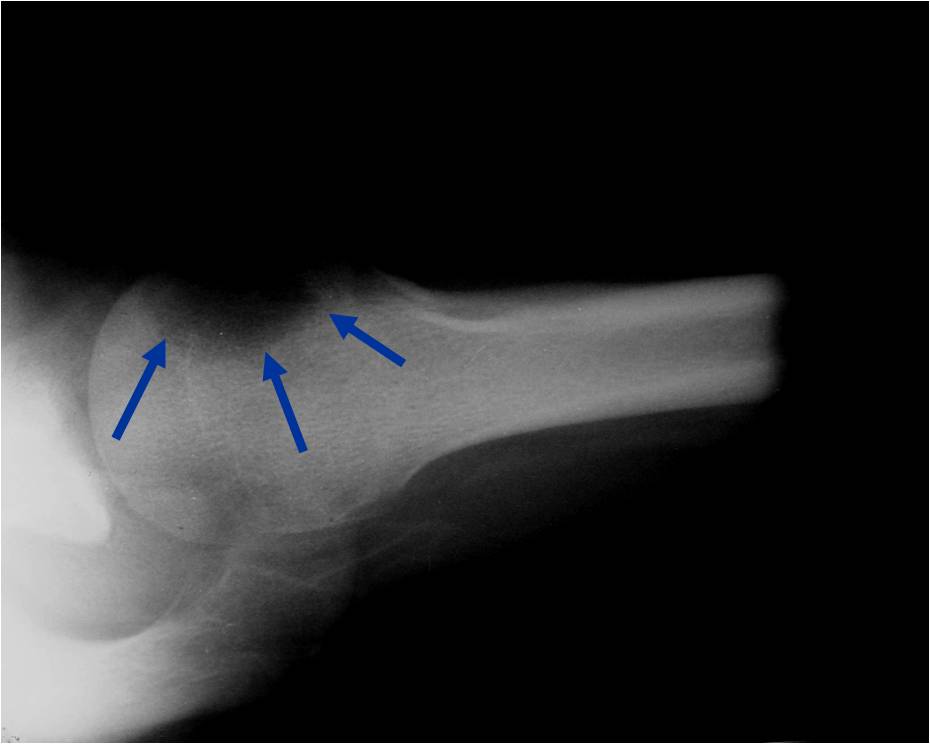
Plain x-ray appearance:
- Geographic lytic lesion IA/IB margin of sclerosis
- Usually Eccentric more often than Central in the bone
- Rarely expansile (rarely penetrates the cortex)
- Calcified chondroid matrix 30%-50% of cases
- Often better detected with a CT Scan
- Periosteal Reaction 30-50% of cases
- Usually occurs in Adjacent Diaphysis/Metaphysis since epiphysis is intraarticular and not surrounded by periosteum
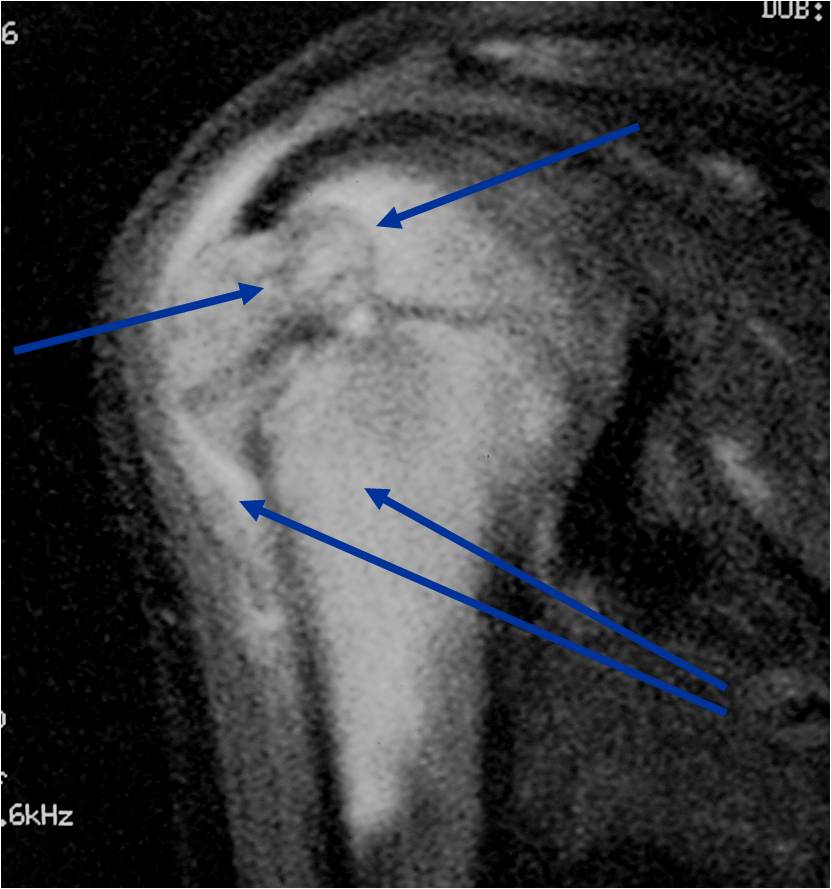
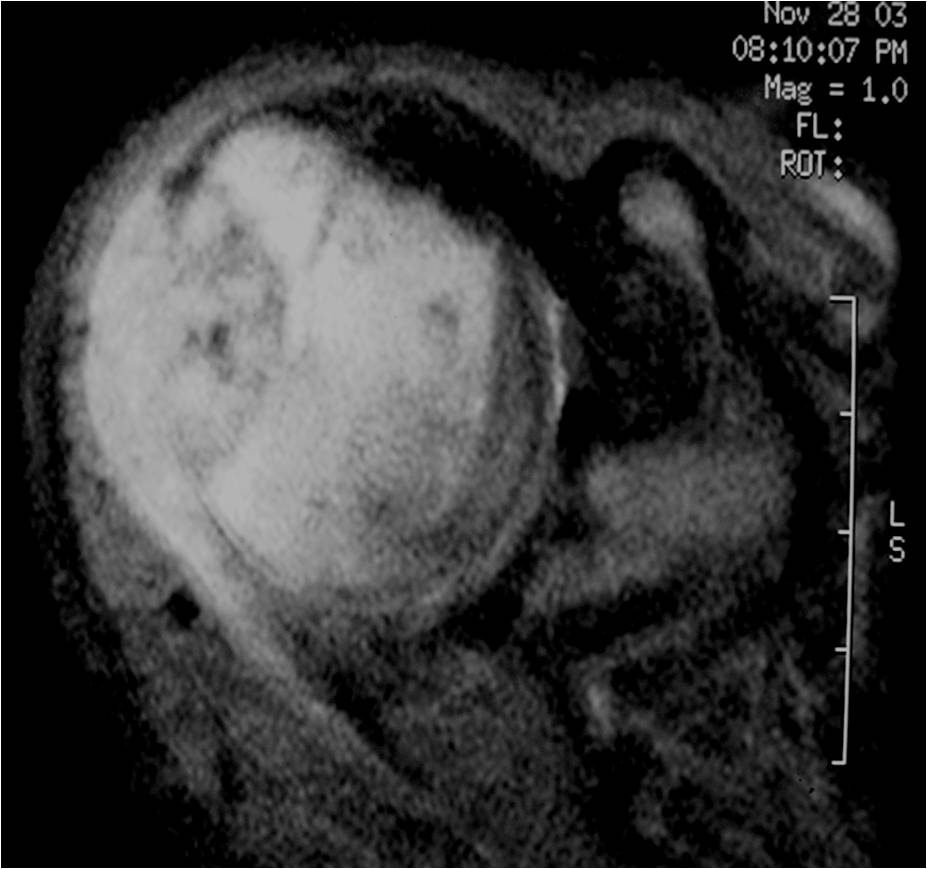
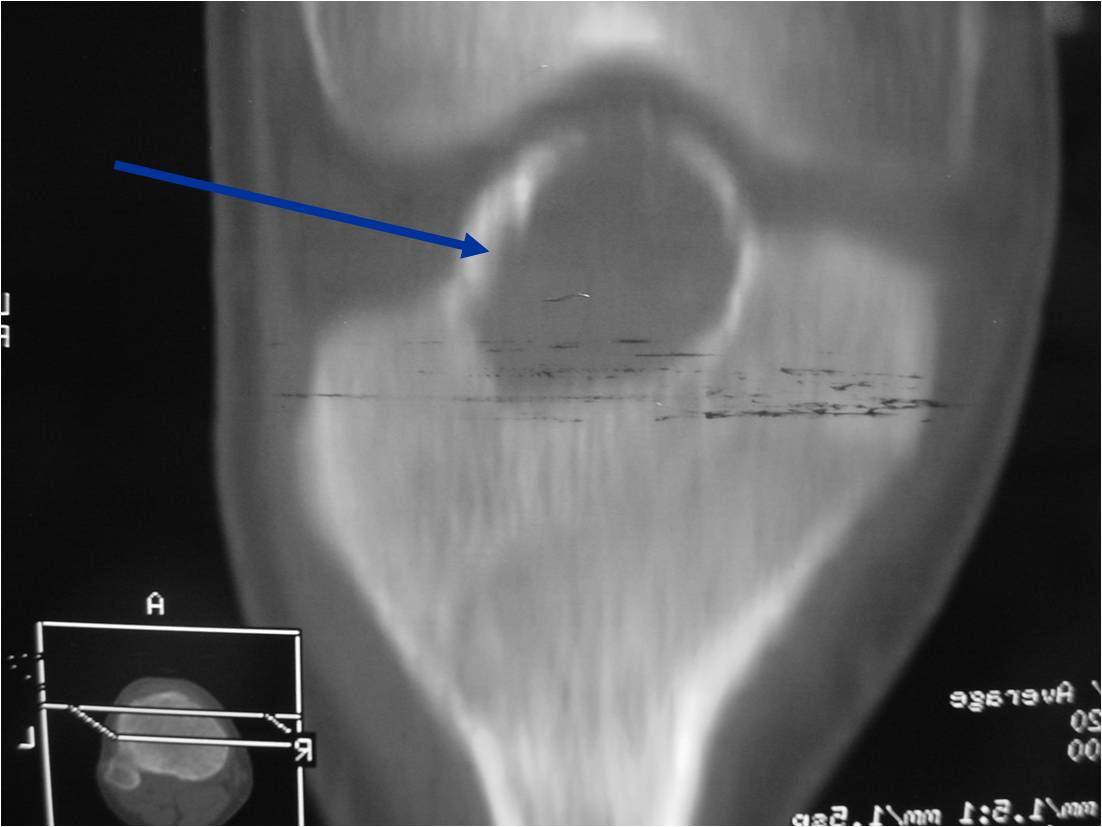
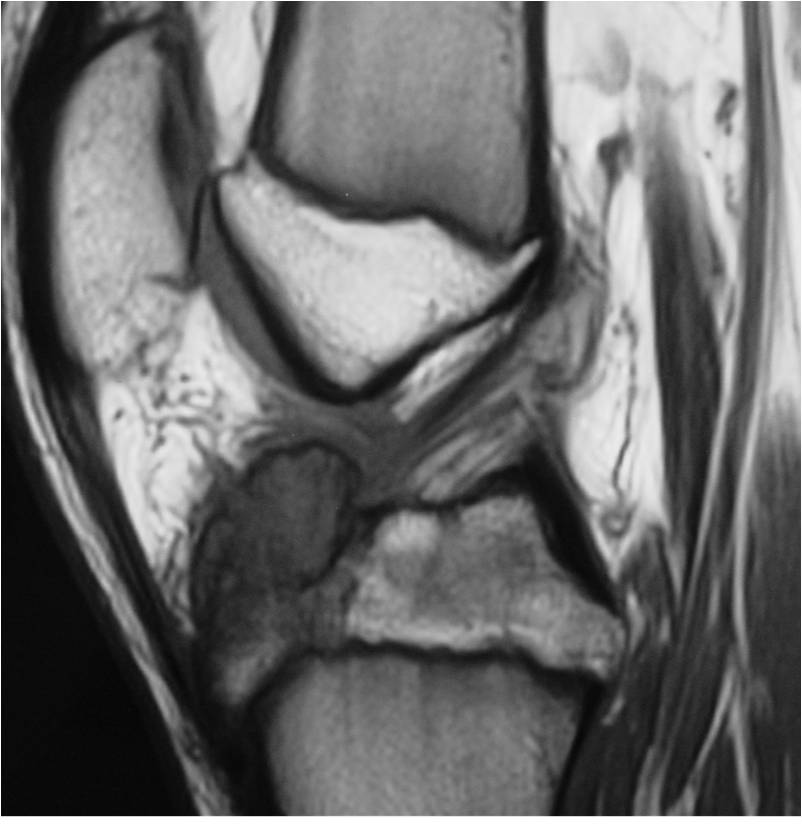
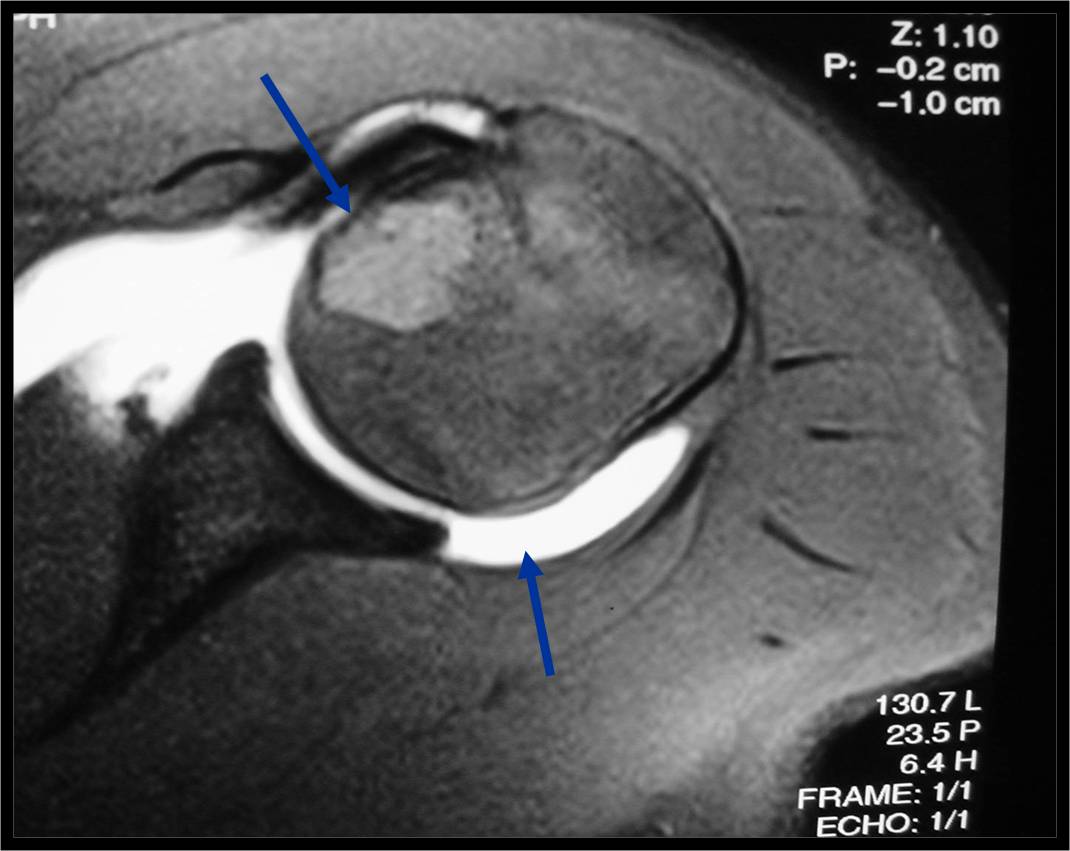
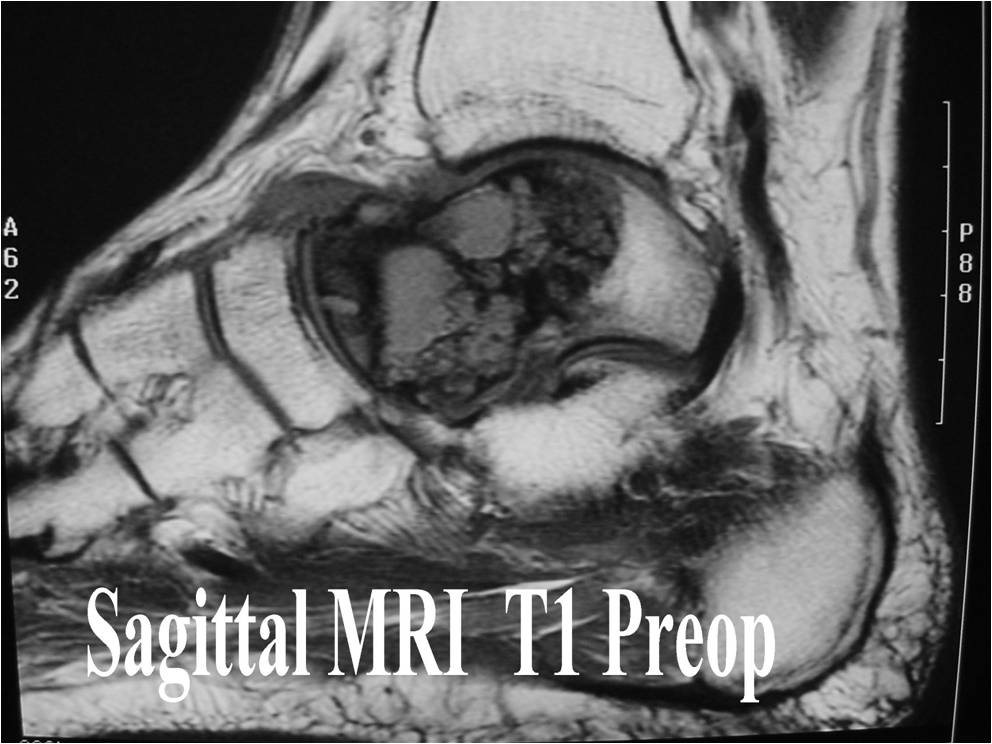
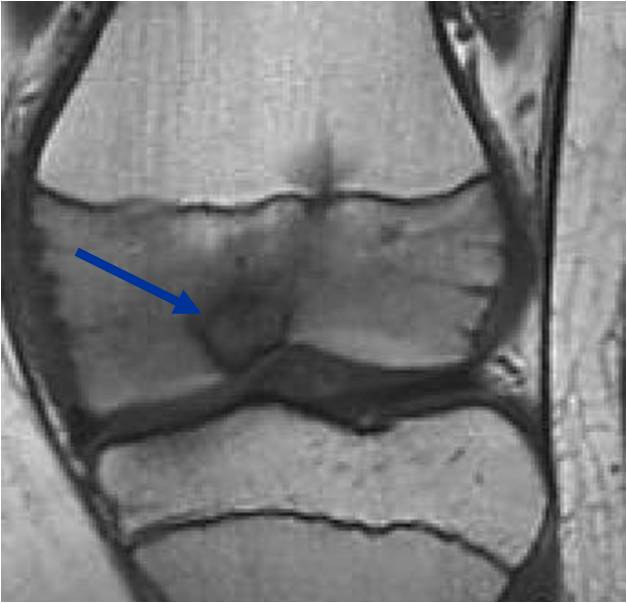
MRI appearance:
- Geographic, well circumscribed lesion in the epiphysis
- Intermediate Signal on T1
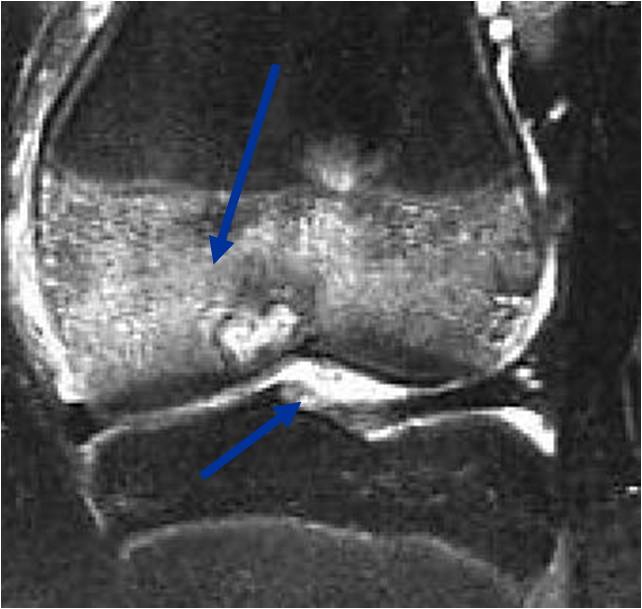
- High signal on T2 mixed with low signal areas (low signal areas proposed to be secondary to lysosomal content of highly cellular areas)
- Fluid/Fluid levels demonstrated in tumors that have undergone ABC change (aneurysmal bone cyst change)
- Extensive Surrounding edema is common
- Joint effusion in 30-50% of cases
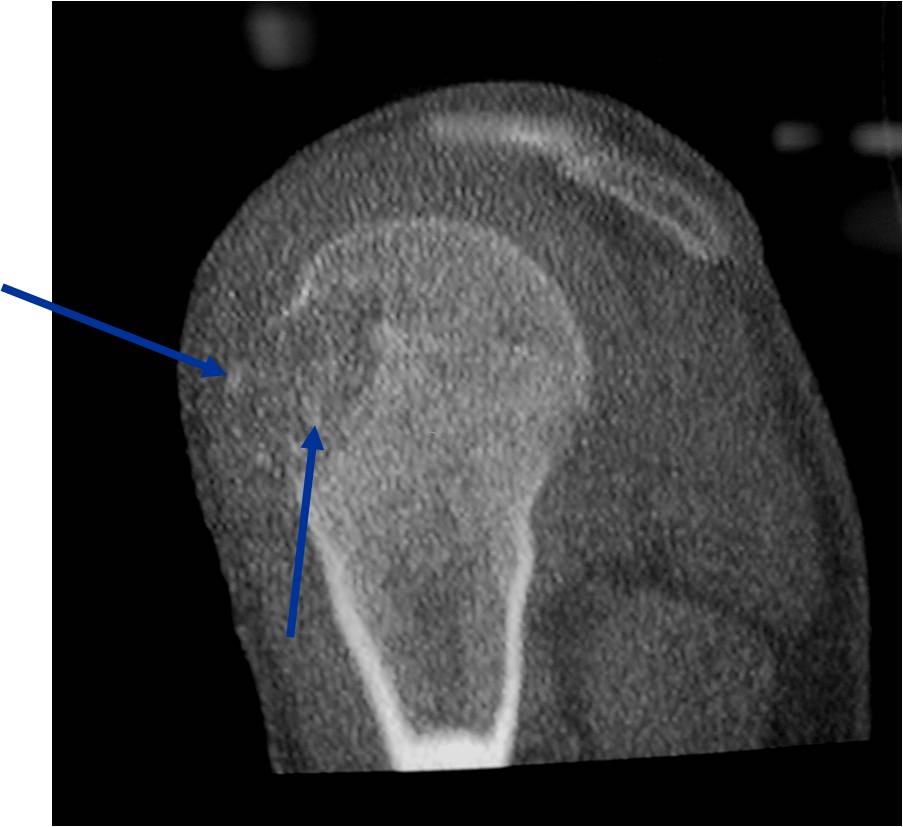
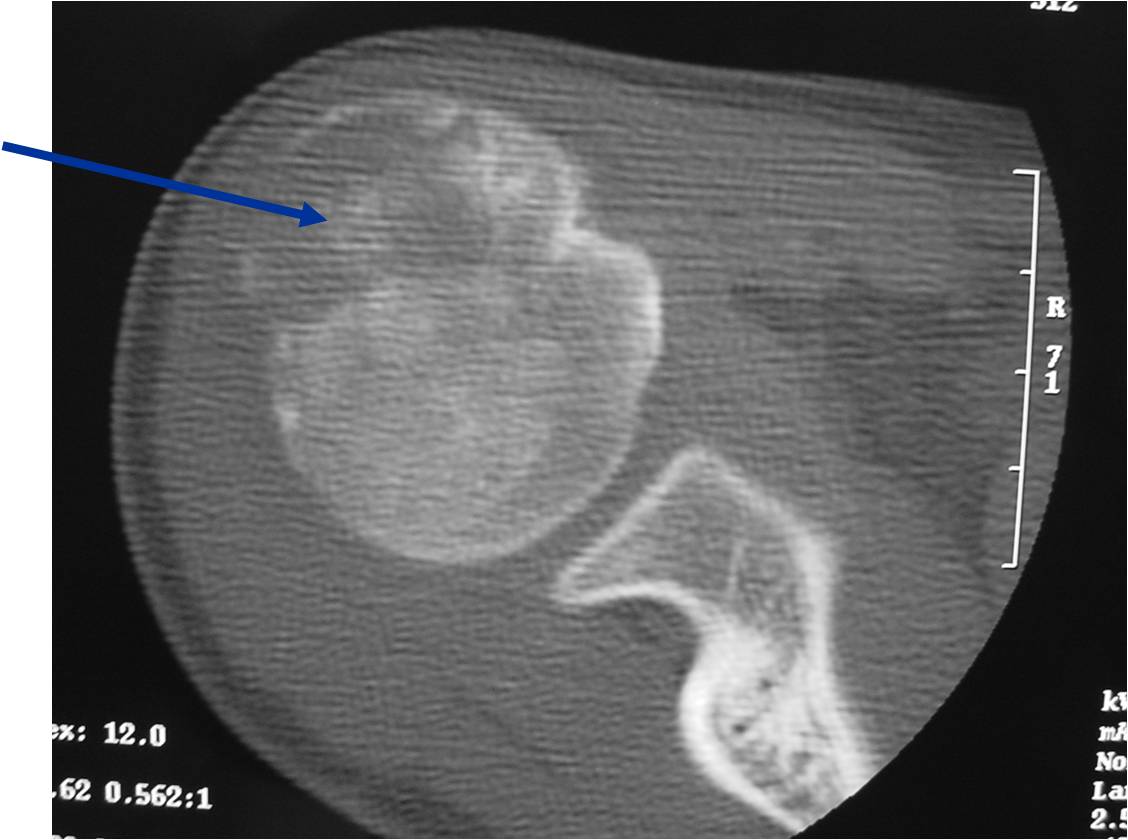
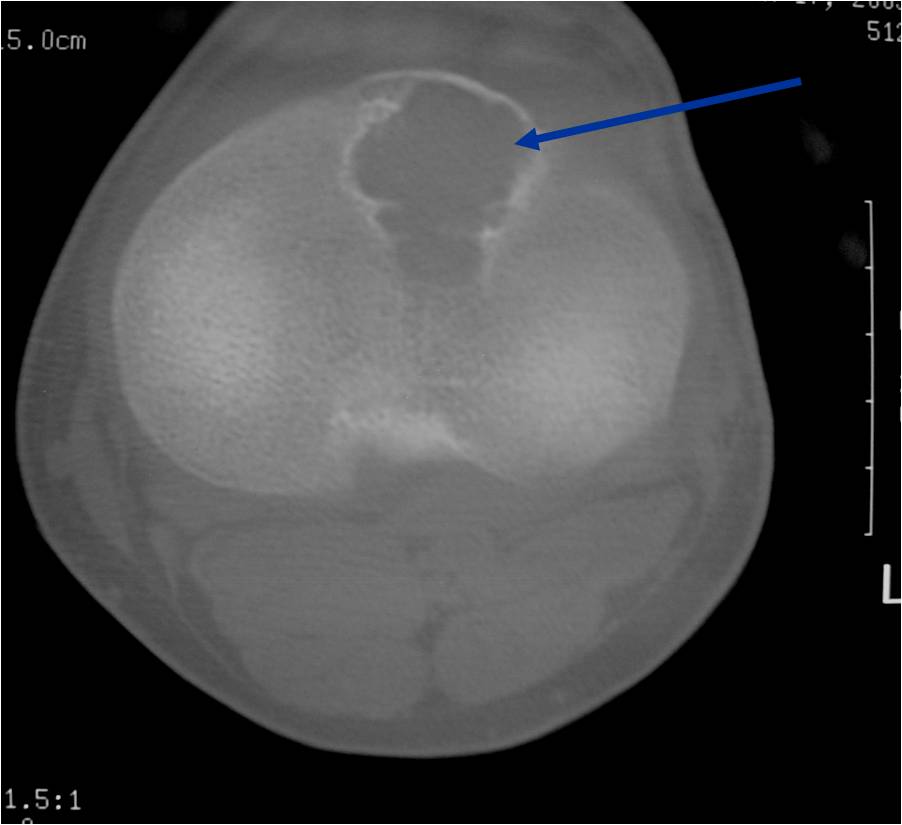
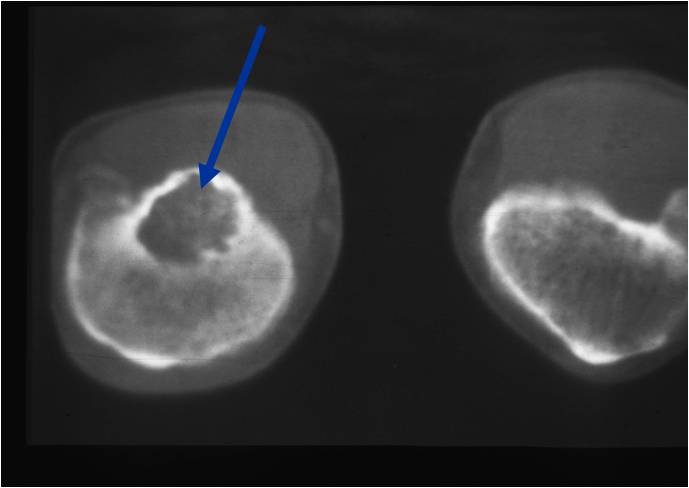
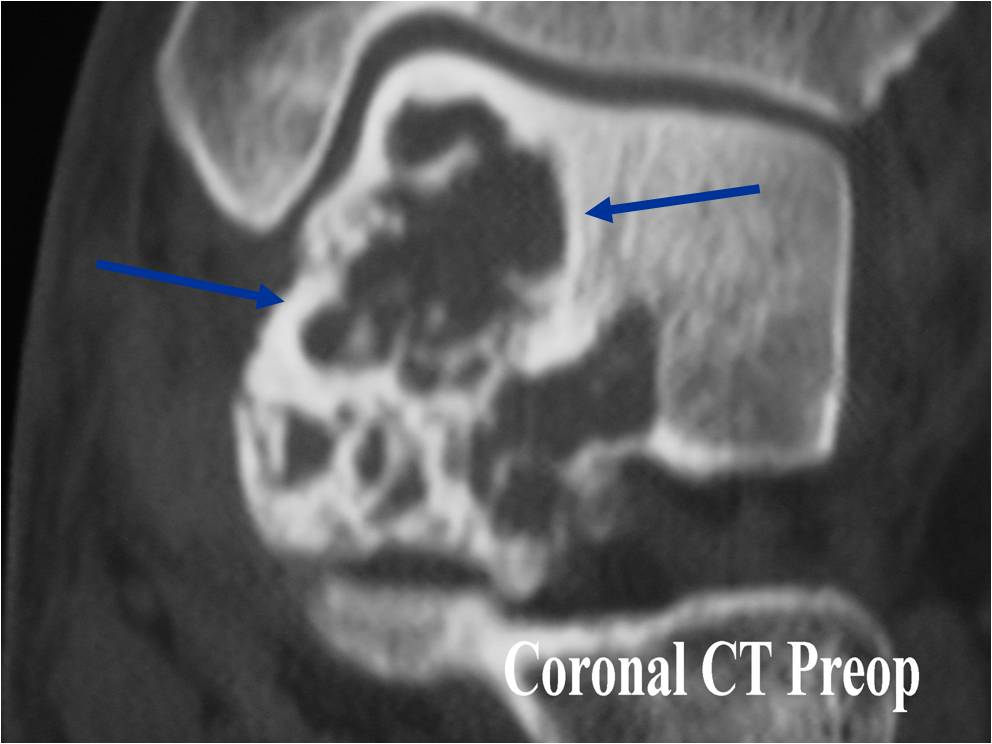
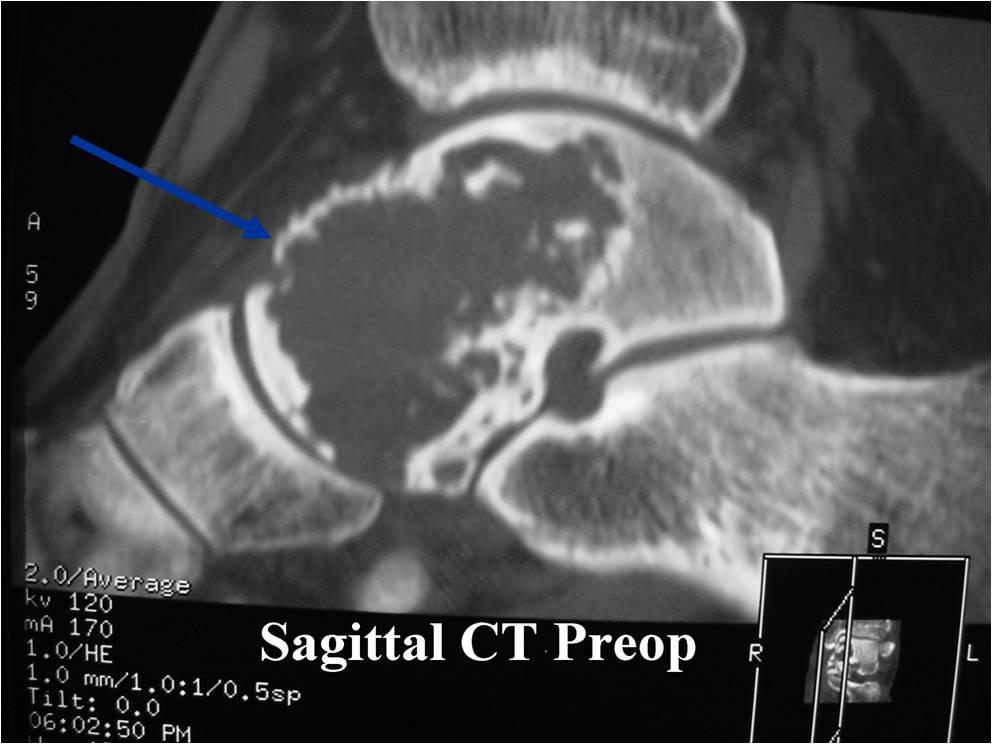
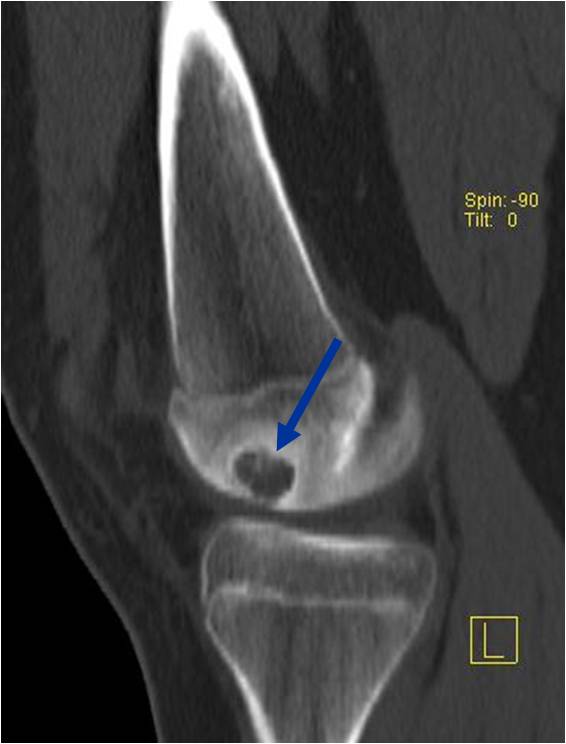
CT appearance:
- Most useful for detecting subtle mineralization not apparent on X-rays
- Useful for identifying intact periosteum around any expansile soft tissue component
- surrounding thin reactive shell of bone/mineralization (Egg Shell Rim of Calcification)
- helps place the tumor in a benign category
- helps evaluate:
- bony quality
- extent of bone and cortical destruction
- whether the subchondral plate of bone adjacent to the articular cartilage has been destroyed or is intact
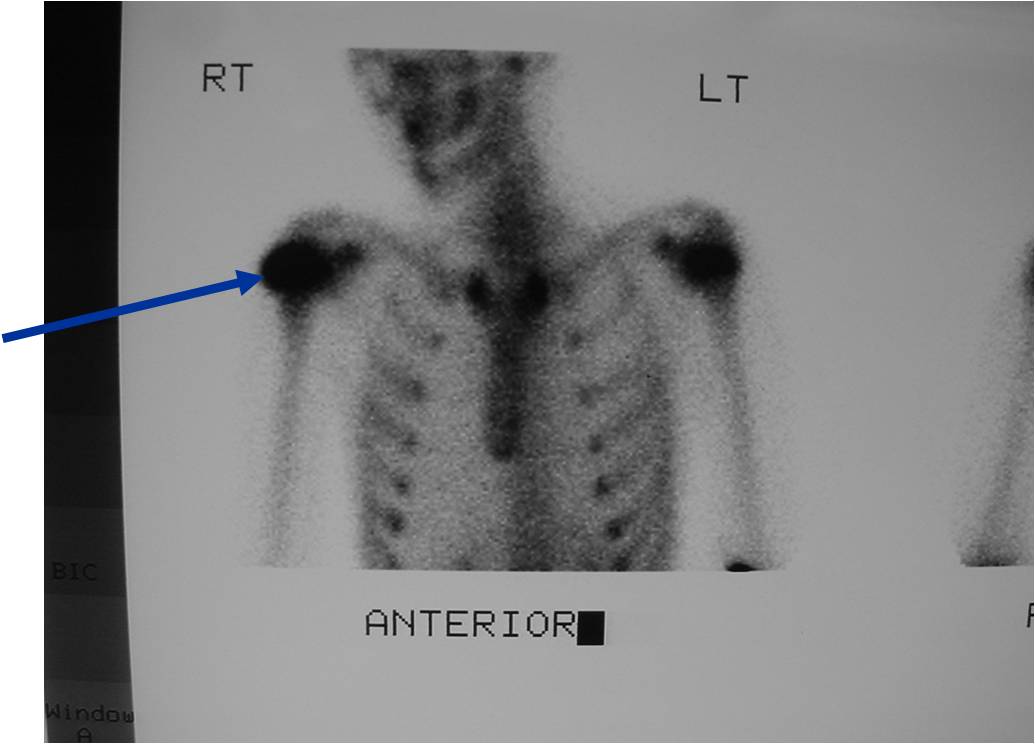
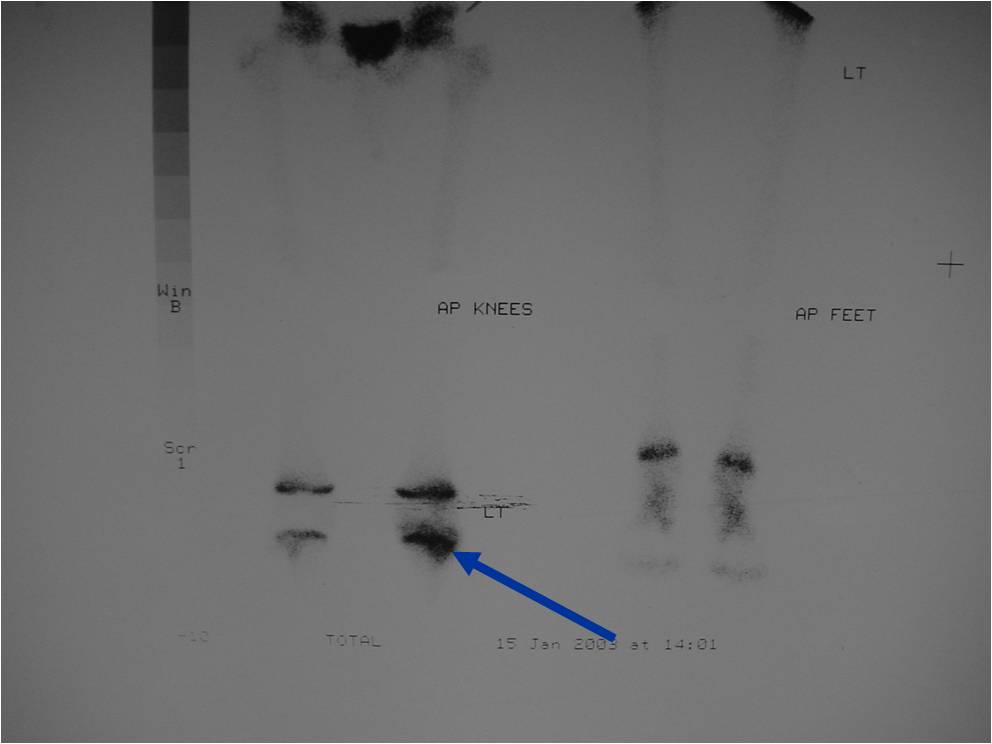
Bone scan: Chondroblastomas demonstrate intense increased uptake on a bone scan
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
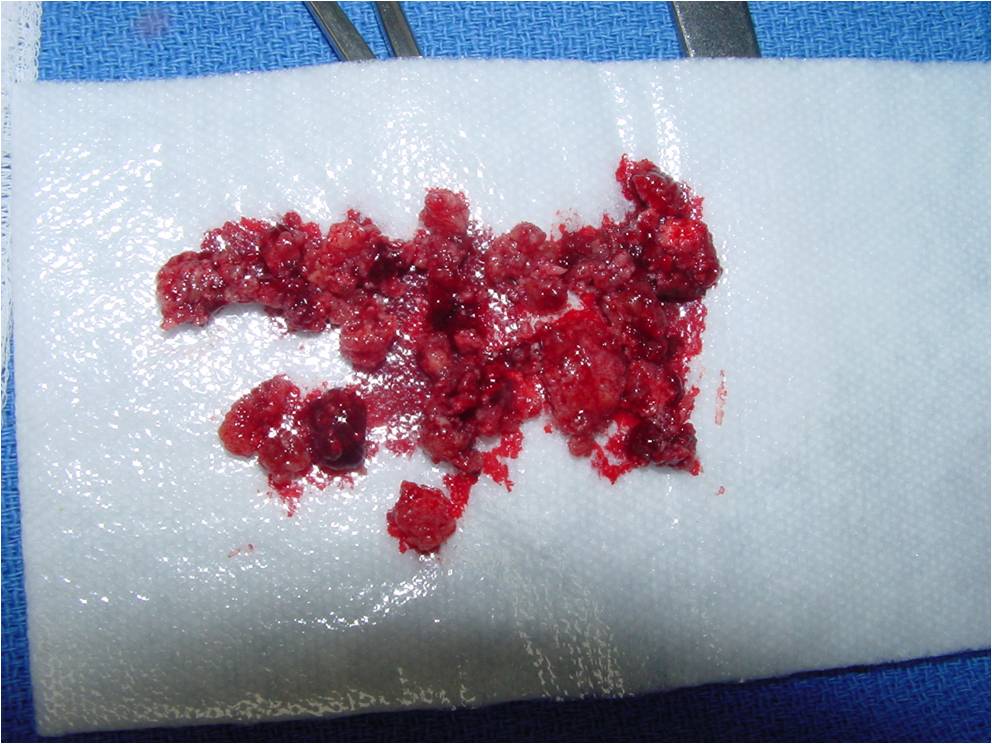
Gross Pathology
- Grossly variable appearance
- Grey/yellow/brown and gritty if has interspersed calcifications
- Interspersed red areas from hemorrhagic necrosis
- May be blue-grey areas from the chondroid matrix
- Rim of sclerotic bone is visible in totally resected specimens
- Lesion may be fully cystic with solid foci of tumor tissue at periphery
- May undergo aneurysmal bone cyst change (ABC change)
| Roll over the images for more information |
 |
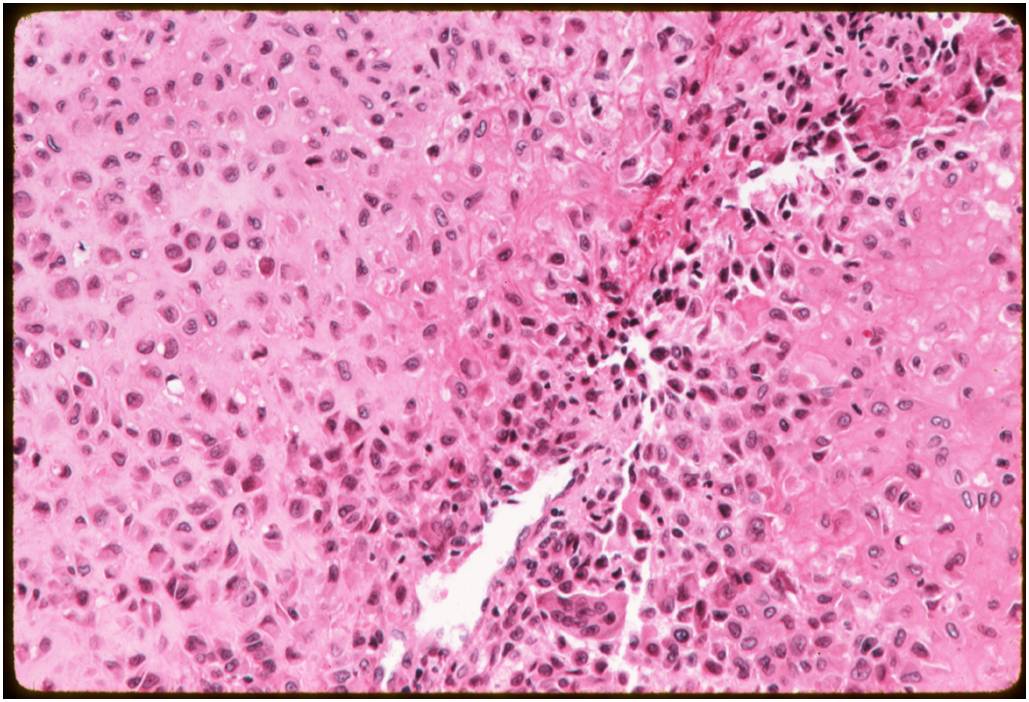
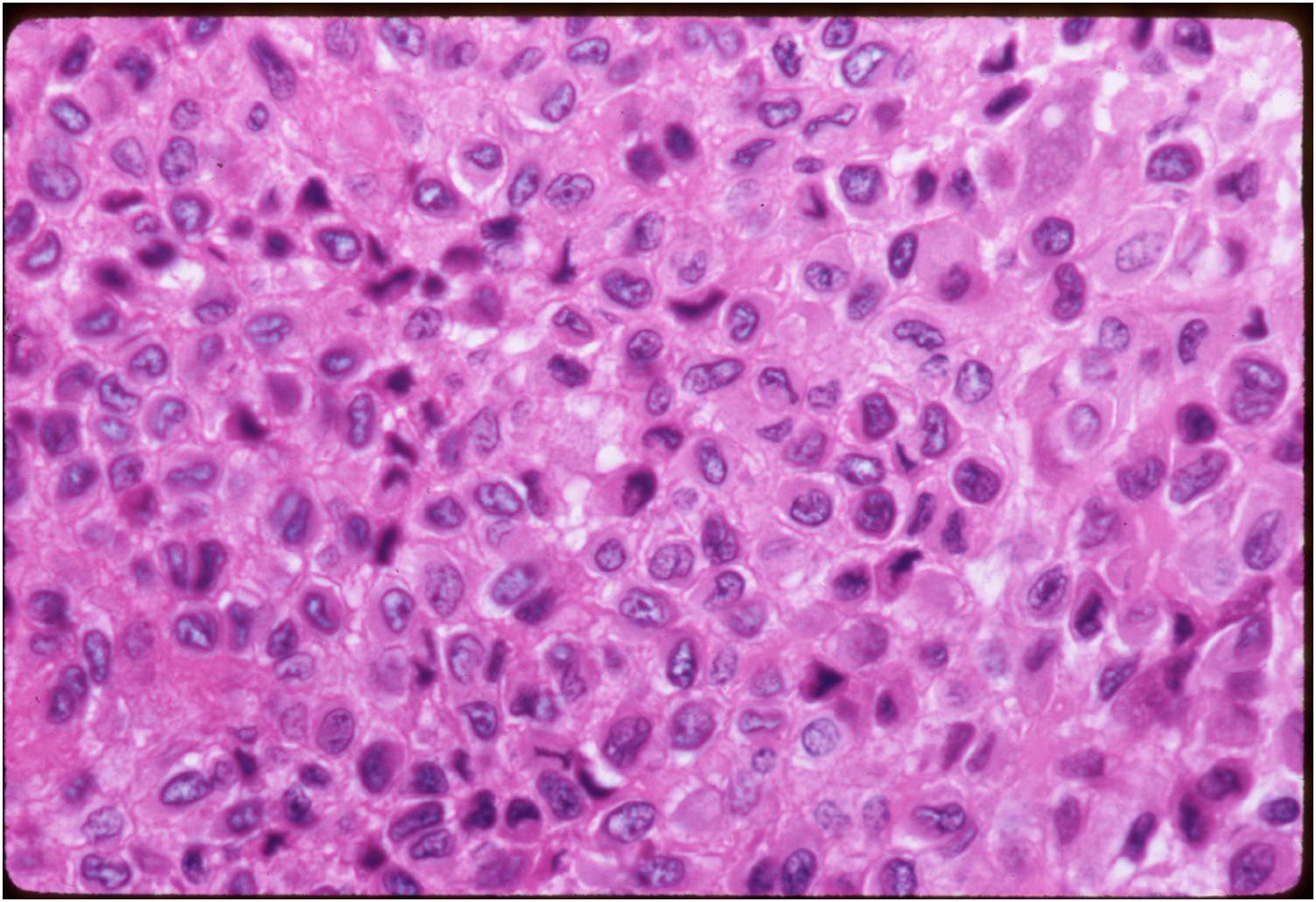
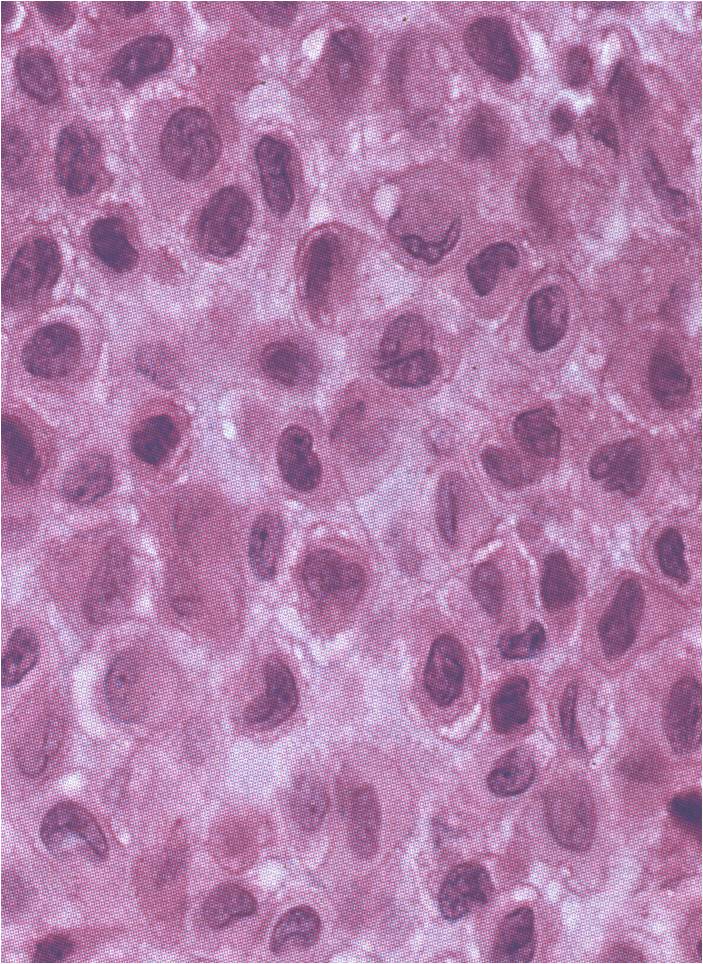
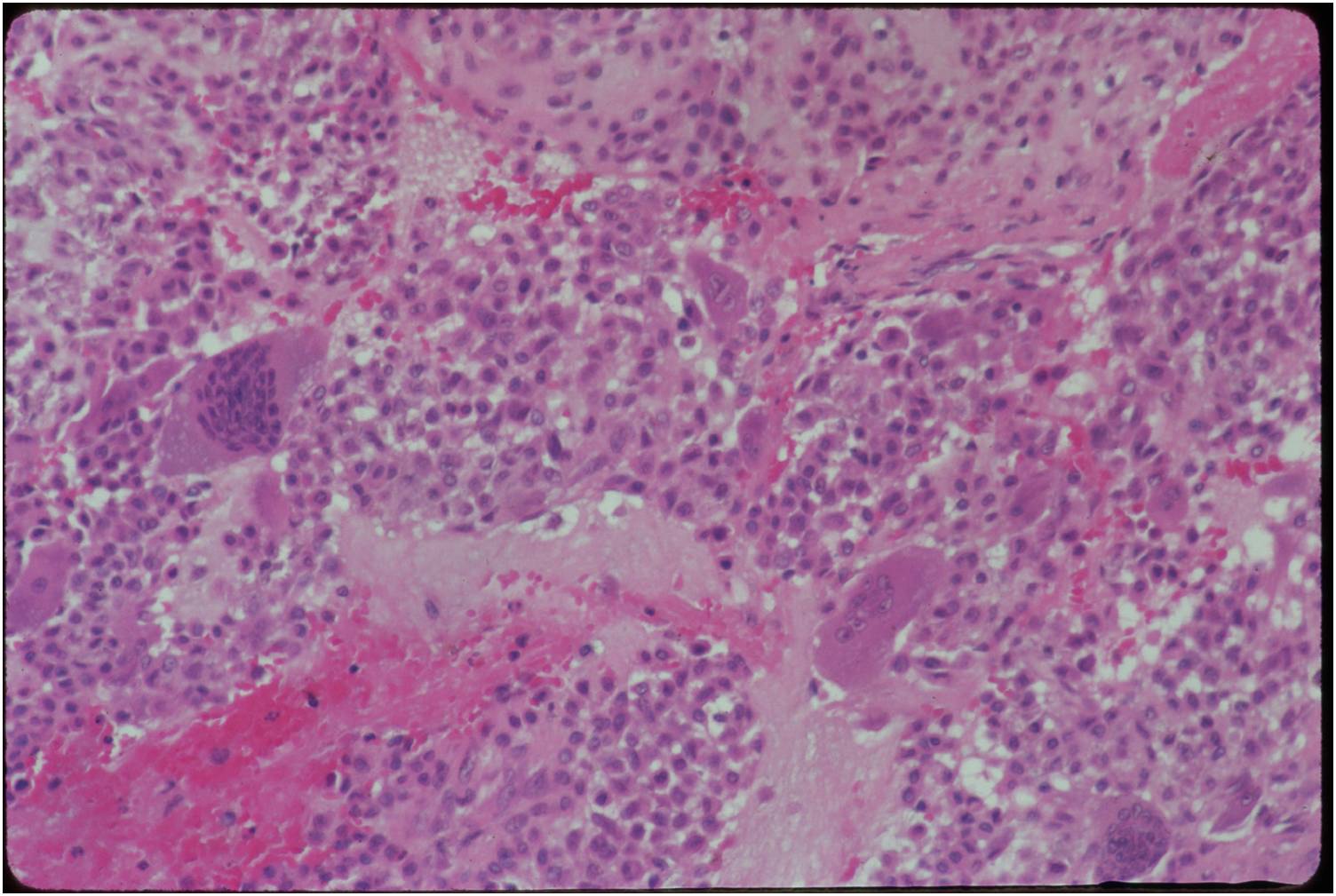
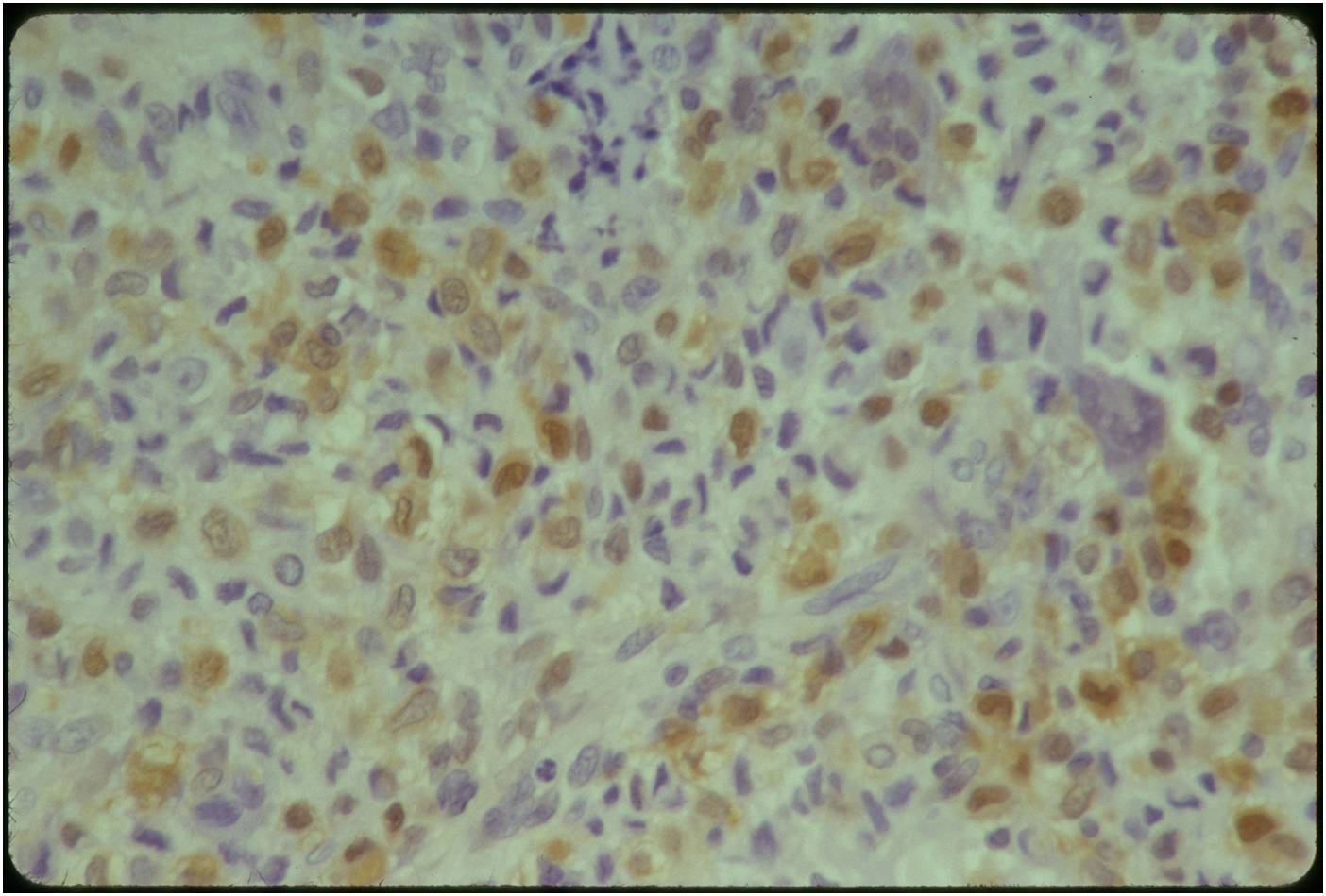
Microscopic Pathology
- Variable appearance depending on percentage of cells, necrosis, cartilage matrix formation and ABC change
- Chondroid matrix in up to 15% of tumor
- ABC component 5-15% of tumors
- The tumor is composed of chondroblasts that have a distinct, thick cell membrane. The thick cell membrane gives it a "Chicken Wire Fence Appearance," especially when the cell membranes are calcified
| Roll over the images for more information |
 |
 |
 |
 |
 |
 |
Biological Behavior
- benign aggressive tumors
- grow aggressively, destroy bone
- can destroy the cortex and grow into the soft tissues
- contained by the periosteum (this differs from a malignant tumor that destroys the cortex)
- EXTREMELY rare cases where chondroblastomas metastasize to the lungs after 30 years
- Metastases may remain stable or may progress and cause death
- Recurrences may occur in the bone or adjacent soft tissue
- Rare cases of multifocal chondroblastomas have been documented (Synchronous involvement of several sites)
- Secondary aneurysmal bone cyst frequently correlated with chondroblastoma
- Chondroblastomas have been reported to transform into fibrosarcoma or osteosarcoma years after being treated with radiation.
Treatment
