General Information
- High grade surface osteosarcoma is a type of high grade osteosarcoma that develops on the surface of the bone from the outer cortex.
- There is none to minimal medullary involvement
- The microscopic pathology is the same as a conventional osteosarcoma and it has the same high potential for metastasizing.
- High grade surface osteosarcoma is the least common type of surface osteosarcoma (Parosteal and periosteal osteosarcomas are more common)
- This is a very rare neoplasm and constitutes <1% of all osteosarcomas
Clinical Presentation
Signs/Symptoms:
- Pain and/or swelling lasting from months to more than a year
Prevalence:
Age:
- 2nd Decade is most common
- Patients have ranged in age from 9 to 62 years
Sites:
- Femur (45%);
- Humerus (26%);
- Fibula (10%);
- Ulna are the most commonly reported sites
Usually arise from the diaphysis or metadiaphysis of the bone
Radiographic Presentation
Plain X-Rays:
- Broad based mass on surface of bone that is partially mineralized (fluffy calcifications/ossification in mass)
- Appearance similar to periosteal osteosarcoma but usually with more ossification
- Matrix mineralization is similar to conventional osteosarcoma with cloudlike opacities
- Amount of mineralization varies
Codman's triangle/Malignant periosteal reaction may be present
- Cortical erosion is usually evident
- Medullary cavity is usually uninvolved
| Roll over the images for more information |
 |
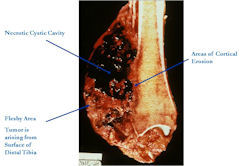
Gross Pathology
- Tumors are bulky, lobulated masses
- Have firm, soft, and hemorrhagic areas
- Dense sclerosis typical of a parosteal osteosarcoma and significant amounts of cartilage typical of a periosteal osteosarcoma is not common
- Cortex usually roughened and eroded
- There may be small foci of intramedullary invasion
| Roll over the images for more information |
 |
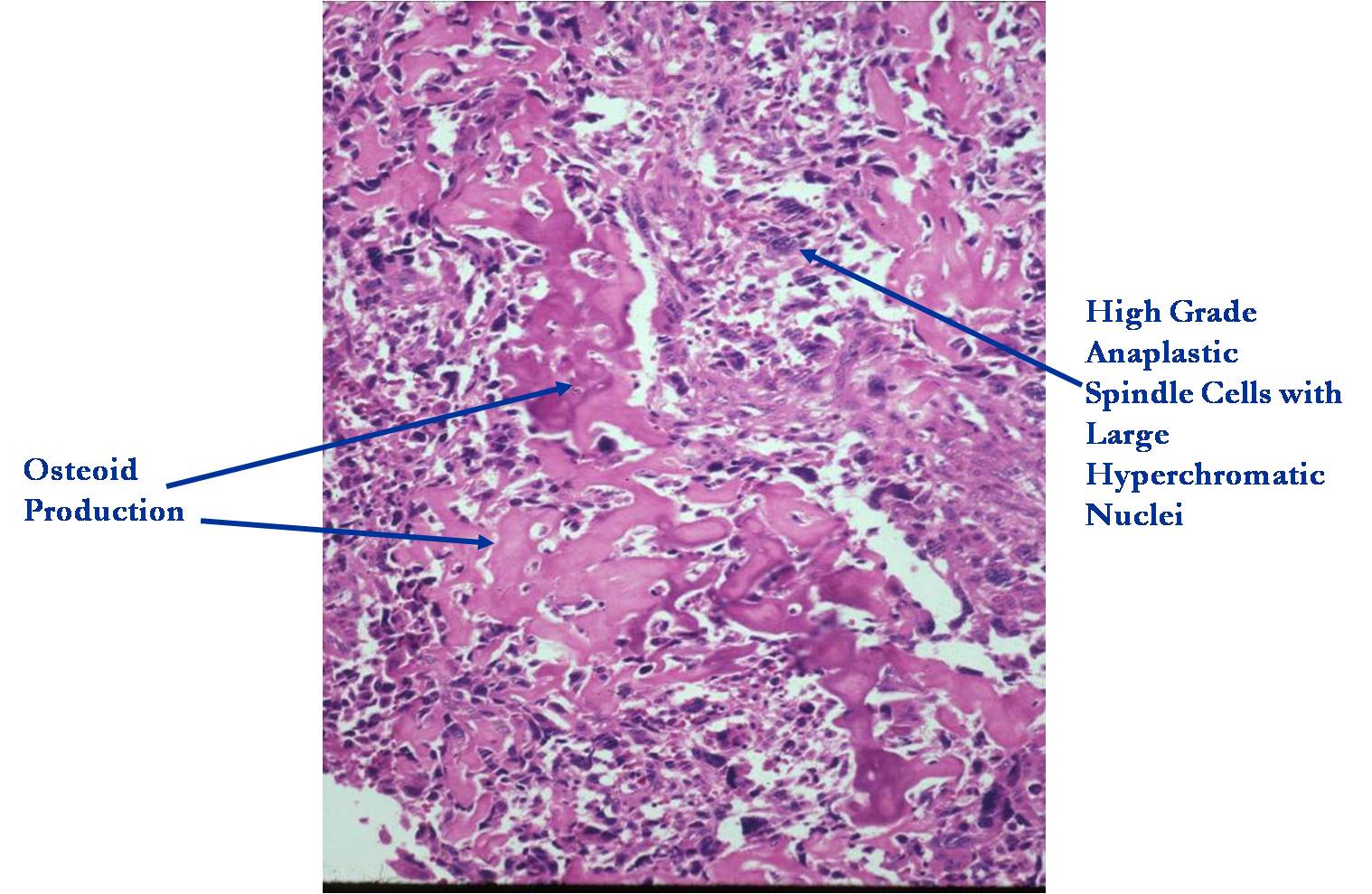
Microscopic Pathology
- The pathology of a high grade surface osteosarcoma is indistinguishable from conventional medullary osteosarcoma
- The lack of medullary involvement distinguishes this tumor from a conventional intramedullary osteosarcoma
- It consists of high grade, anaplastic, pleomorphic spindle cells producing osteoid and immature bone that is deposited in a lace-like manner
| Roll over the images for more information |
 |
Differential Diagnosis of High Grade Surface Osteosarcoma
- Parosteal Osteosarcoma
- Dedifferentiated Parosteal Osteosarcoma
- Periosteal Osteosarcoma
- Intramedullary Osteosarcoma with large soft tissue component
- (please refer to descriptions of parosteal and periosteal osteosarcoma)
- Differentiating a high grade surface osteosarcoma from a conventional osteosarcoma is not important prognostically. They are essentially both treated in a similar manner as of 2008.
Biological Behavior
- The biological behavior of a high grade surface osteosarcoma is similar to a conventional intramedullary osteosarcoma
- There is a high risk for developing metastatic disease.
- The most common site for developing metastases is the lungs.
- The second most common site is other bones.
Treatment
The Treatment usually follows the same protocols as that used for conventional intramedullary osteosarcoma. Often COG (Children’s Oncology Group) protocols are employed.
Preoperative (induction) chemotherapy:
- Adriamycin (doxorubicin)
- Cisplatinum (cisplatin)
- High Dose Methotrexate (HDMTX)
- Ifosfamide/Etoposide in some regimens
- (2 cycles and then surgery)
Surgery:
- Wide Surgical Resection/Limb Salvage for most patients
- Amputation
Postoperative Chemotherapy:
- Usually 4 cycles postoperatively
- Usually same medications as preoperative regimen although may be modified for various reasons such as a poor response to the preoperative chemotherapy medications
Prognosis
- Tumor has a great propensity for distant metastasis
- Metastases occur in 80% of patients treated by excision alone
- Lungs and other bones are most common sites
- Overall 5-year survival rate depends on site, size, resectability, presence of metastasis. Survival is similar to conventional intramedullary osteosarcoma.
