Leiomyosarcoma
GENERAL INFORMATION
Leimyosarcoma is a rare malignant spindle cell tumor (sarcoma) composed of cells which demonstrate smooth muscle differentiation. Almost 50% percent affect the retroperitoneum. Leiomyosarcoma have been subdivided into 3 categories: leiomyosarcoma of peritoneum, leiomyosarcoma of deep soft tissues outside the peritoneum and leiomyosarcoma of subcutaneous tissues. Prognosis will depend grade, size and location of the tumor.
CLINICAL DATA
Affect age group of 40 to 60 years.
Represents almost 9% of all soft tissue sarcomas
Present often as a painless mass
Sites
Retroperitoneum (first place with almost 50%)
Thigh (second most common area)
Subcutaneous distribution (6%)
Can arise from the wall of the blood vessel (location of smooth muscle)
DIFFERENTIAL DIAGNOSIS
Malignant fibrous histocytoma
Dedifferentiated liposarcoma
Angiomyolipoma
Mesenteric fibromatosis
Fibrosarcoma
Malignant Peripheral Nerve Sheath Tumor
Monophasic synovial sarcoma
CLINICAL PRESENTATION
Signs/Symptoms
Slow-growing mass
Soft tissue mass that may be or not be painful, and tender (retroperitoneum)
Usually do not develop symptoms until the mass grows more than 10 cm ( retroperitoneum)
Almost all tumrs outside of the peritoneum are painless
Prevalence
Preference for women
Except subcutaneuous tissue, preference for male.
Third most common soft tissue sarcoma.
Mostly middle-aged and older adults
Small subset of children (immunosuppressed, HIV)--->deep soft tissue other than retroperitoneum
Site
Almost 50% of the cases located in retroperitoneal area
Extremities, particulary lower/thigh area
RADIOGRAPHIC PRESENTATION
Plain x-ray
No specific radiological features (demonstrate soft tissue mass)
Calcifications are rare
CT
Nonspecific mass (Fig. 1)
Frequently demonstrate areas of low attenuation,--->heterogeneous areas (hemorrhage, necrosis, or cystic change)
 Fig. 1 Axial CT reconstruction of a leiomyosarcoma of the thigh located in the medial compartment, isointense to muscle
Fig. 1 Axial CT reconstruction of a leiomyosarcoma of the thigh located in the medial compartment, isointense to muscle
MRI
Nonspecific nonfatty mass (Fig. 2,3)
Large heterogeneous mass (Fig. 4, 5, 6)
Isointense to skeletal muscle on T1W
Usually heterogeneous on T2W SE
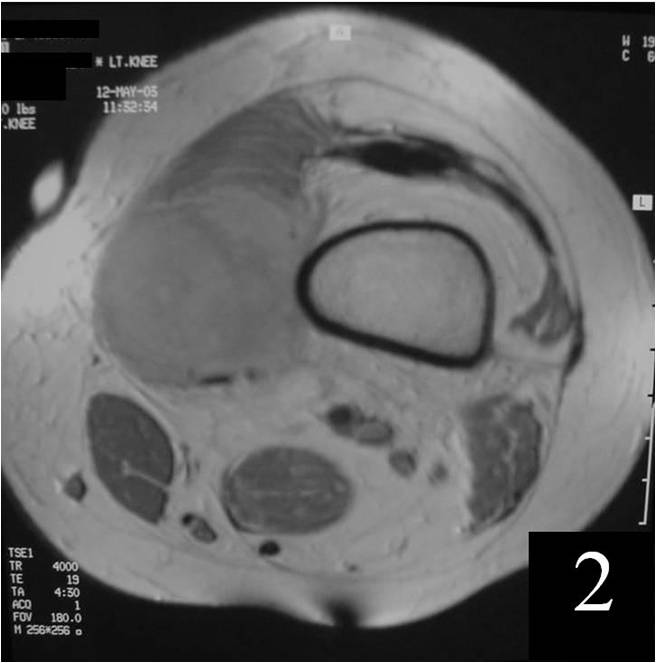 Fig. 2 T1W MRI of a leiomyosarcoma of the thigh shows a mass isointense to muscle
Fig. 2 T1W MRI of a leiomyosarcoma of the thigh shows a mass isointense to muscle
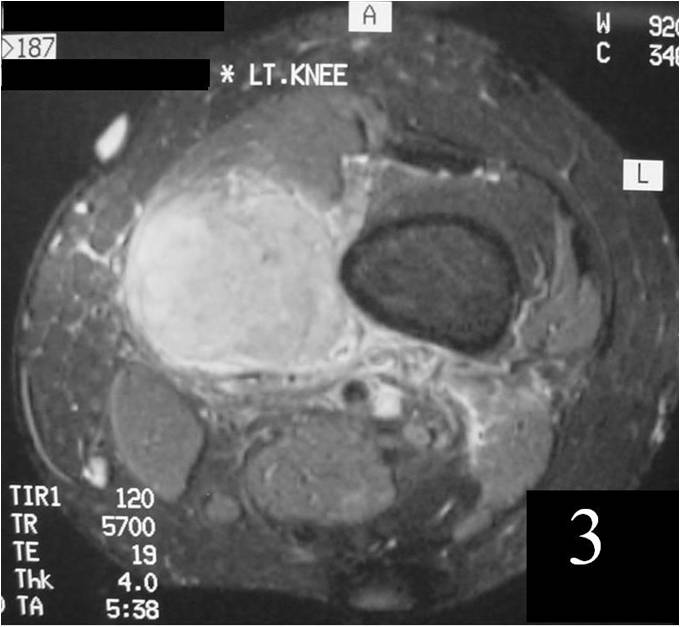 Fig. 3 T2W MRI with contrast shows enhancement of a leiomyosarcoma in medial compartment of the thigh
Fig. 3 T2W MRI with contrast shows enhancement of a leiomyosarcoma in medial compartment of the thigh
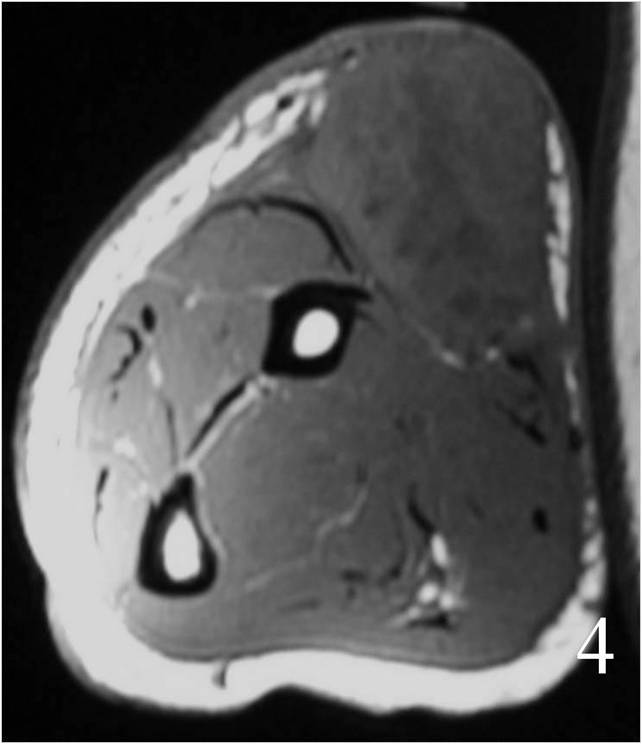
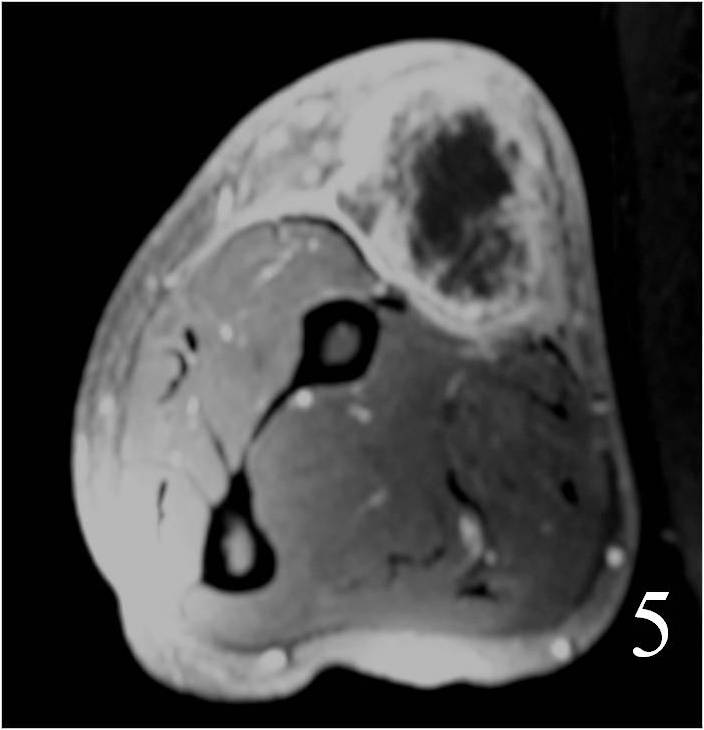
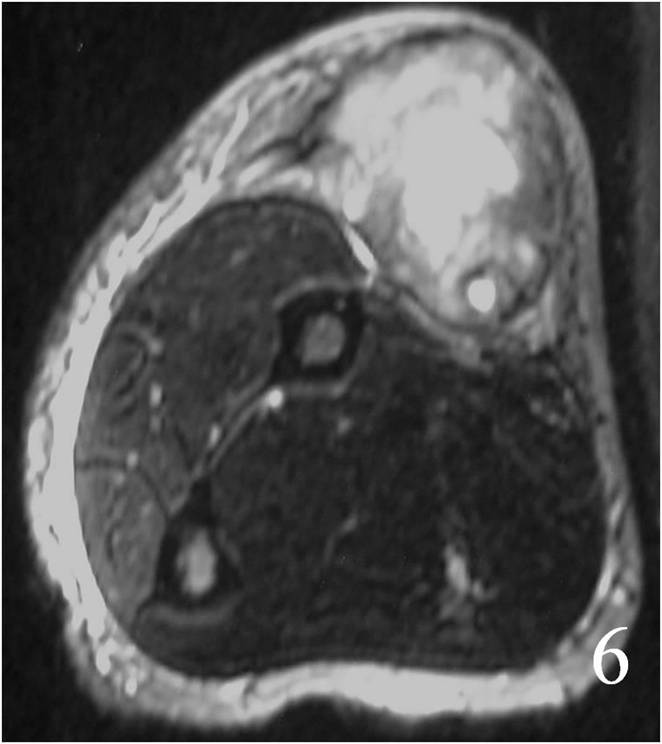 Fig. 4 MRI of a leiomyosarcoma of the forearm shows a mass isointense to muscle on T1W image, heterogeneous on T2W (Fig. 5) and enhances with contrast T1W fat suppressed (Fig. 6)
Fig. 4 MRI of a leiomyosarcoma of the forearm shows a mass isointense to muscle on T1W image, heterogeneous on T2W (Fig. 5) and enhances with contrast T1W fat suppressed (Fig. 6)
PATHOLOGY
Gross
Usually gray-white to fleshy colored
In retroperitoneum and other deep soft tissues:
Cystic changes
Hemorrhage
Necrosis (less in subcutaneous tissue)
Microscopic
Large variation in differentiation, from obvious smooth muscle differentiation to an appearance similar to MFH (Fig. 7,8)
Moderately cellular, with elongated cells and eosinophilic cytoplasm
Cells are arranged in fascicles, with giant cells (giant cells often resemble osteoclasts)
The nuclei look elongated and can have an appearance similar to a corkscrew with round ends
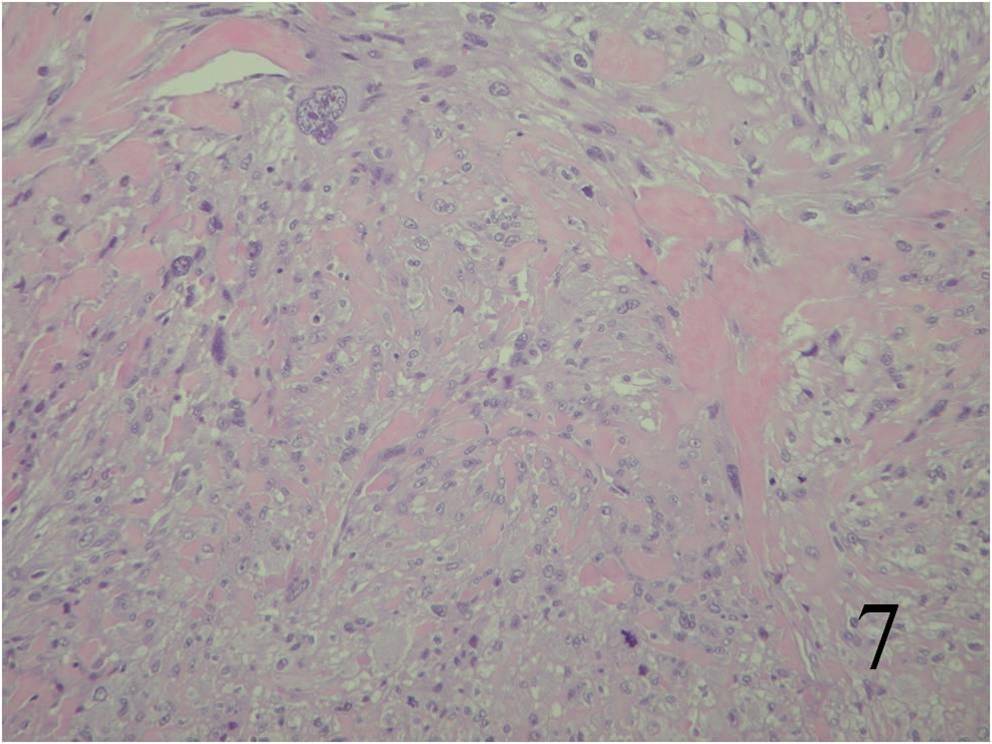
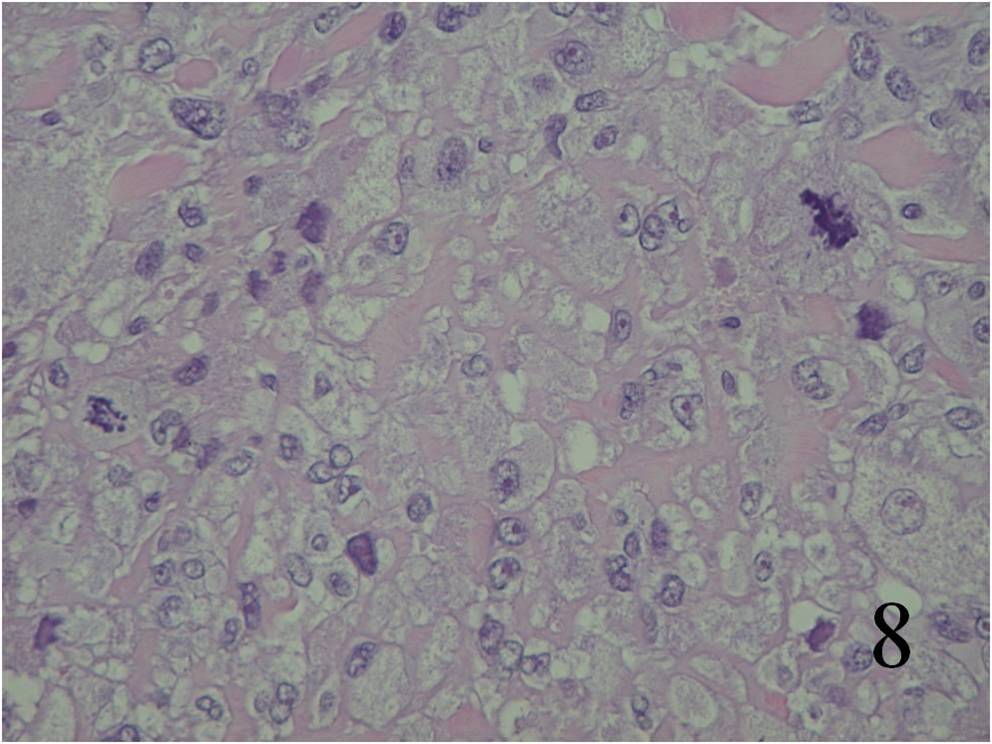
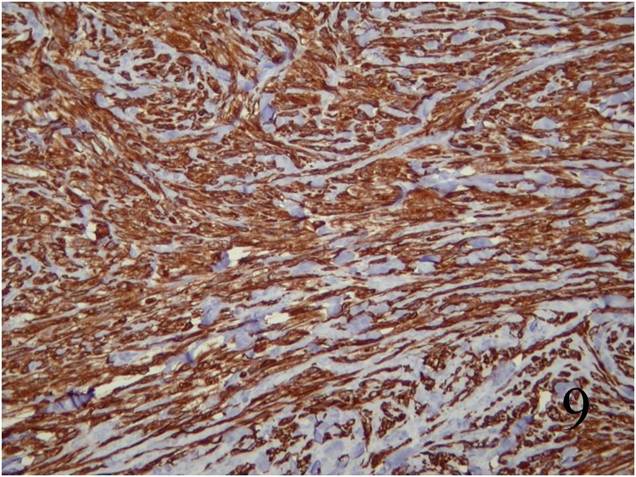
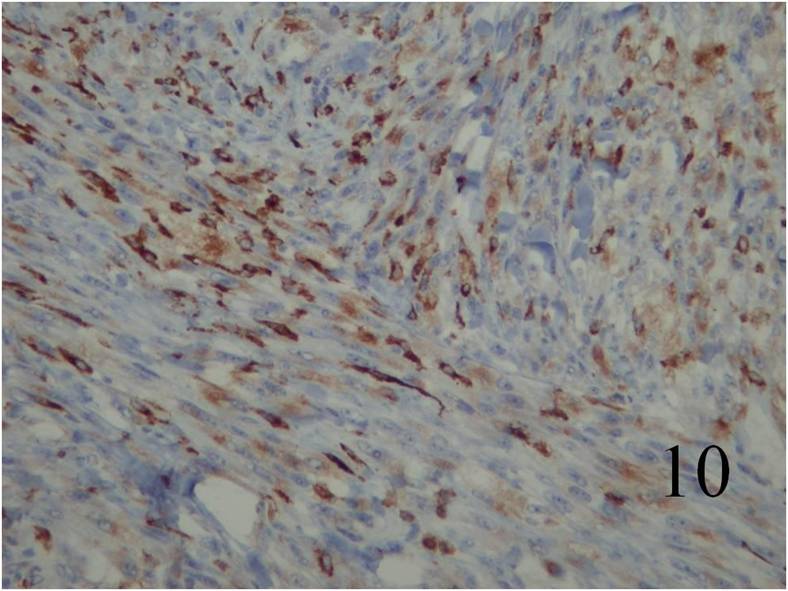 Fig. 7 Microscopic: Low and High (Fig. 8) power magnification of a leiomyosarcoma showing palisading spindle cells; with eosinophilic cytoplasm. Immunohistochemical stains for leiomyosarcoma are positive stain for actin (Fig. 9) and desmin (Fig. 10)
Fig. 7 Microscopic: Low and High (Fig. 8) power magnification of a leiomyosarcoma showing palisading spindle cells; with eosinophilic cytoplasm. Immunohistochemical stains for leiomyosarcoma are positive stain for actin (Fig. 9) and desmin (Fig. 10)
IMMUNOHISTOCHEMISTRY
Desmin and Actin are positive (Fig. 9,10 - above)
Vimentin Positive
Keratin negative
PROGNOSIS
Biological Behavior
Tumors located in an extremity have 50% survival at 5 years.
Retroperitoneal tumors have 25-35% 5 year survival
Earlier diagnosis with deep soft tissue masses and subcutaneous tumors compared to retroperitoneal tumors
More easily noticeable
Less aggressive
Smaller size
Usually a prolonged period of time for diagnosis in retroperitoneoum
Retroperitoneal lesions: 25-35% survival at 5 years.
Extremely aggressive
Invade neighboring organs
Grow more than 10 cm in Ø more than 1,500 gr
Often metastasize to:
Lung
Liver
Bone
Other soft tissues
Lymph nodes
TREATMENT
If is possible, wide resection and postoperative radiation whenever feasible (Fig. 11, 12)
If unresectable amputation
If not amenable to amputation, palliative chemotherapy and/ or radiotherapy can be implemented.

 Fig. 11 Wide resection of subcutaneous leiomyosarcoma of the hand and skin grafting repair of the defect (Fig. 12)
Fig. 11 Wide resection of subcutaneous leiomyosarcoma of the hand and skin grafting repair of the defect (Fig. 12)
