GENERAL INFORMATION
A neurofibroma is a benign tumor of the peripheral nerves, also known as solitary neurofibroma. Neurofibromas can arise as solitary entities or as part of a syndrome, namely neurofibromatosis. Neurofibromatosis is a genetic disease where patients develop multiple peripheral nerve tumors (neurofibromas and schwannomas) as well as cutaneous manifestations. A neurofibroma is not related to fibromatosis which is an entirely different entity
CLINICAL DATA
•
Benign peripheral nerve tumor
•
May be a single lesion
•
Develops during childhood
•
Close to 5% can transform to MPNST usually only in setting of neurofibromatosis
•
As an isolated tumor (not in setting of neurofibromatosis)
o
Non-familial incidence
o
Little malignant change
o
Little recurrence
o
More common
•
These are superficial tumors of the dermis:
o
Orbit
o
Face
o
Neck
o
Back
o
Inguinal area
DIFFERENTIAL DIAGNOSIS
•
MPNST
•
Schwannoma (neurileoma)
•
Neurofibroma
CLINICAL PRESENTATION
Sign/Symptoms
•
Slow-growing and usually small
•
Painless nodule
Prevalence
•
No predilection for sex or race
•
Somewhat rare
•
Usually between 20 and 30 years
•
Other age could be affected as well
Site
•
Distributed throughout body surface
RADIOGRAPHIC PRESENTATION
X ray
o May reveal soft tissue mass
o Displacement of neurovascular bundle may also be apparent
CT
o Fusiform shape
o Nerve can often be seen entering/exiting the mass
o Perilesional rim
MRI
o Tubular structure
o Discrete margins, but sometime noticeable low signal intensity rim
o Attenuation lower than the muscle
o Signal intensity similar to or higher than skeletal muscle in T1W
o High signal intensity in T2W
 Fig. 1 Axial MRI of a large neurofibroma of lower extremity
Fig. 1 Axial MRI of a large neurofibroma of lower extremity
PATHOLOGY
Gross
•
Gray-white
•
Deep tumors are often large
•
Can resemble a “bag of worms” refrred to as a plexiform neurofibroma
•
Lack secondary degenerative changes
o
Found in schwannomas
•
If found in major nerves
o
Expand structures in fusiform manner
o
Normal nerve can be seen entering/exiting
o
If contained by epineurium--->Possesses true capsule
o
Usually appear circumscribed but are nonecapsulated
 Fig. 2 Gross photograph of gray-white ovoid specimen after resection
Fig. 2 Gross photograph of gray-white ovoid specimen after resection
Microscopic
•
Interlacing bundles of cells
o
Elongated cells
Wavy, dark-staining nuclei
Intimately associated with collagen
Small to moderate amounts of mucoid separate cells and collagen
o
Stroma of tumor dotted with occasional
•
Mast cells
•
Lymphocytes
•
Sometimes xanthoma cells
•
May be more cellular
o
With schwann cells, but no biphasic pattern
o
Uniform collagen matrix devoid of mucosubstances
o
Cells arranged in fascicles, whorls, or storiform pattern
o
May contain Antoni A areas
o
Not encapsulated so can be distinguished from schwannoma
o
Involves the nerve fascicles; does not arise at periphery like a schwannoma and displace the fascicles
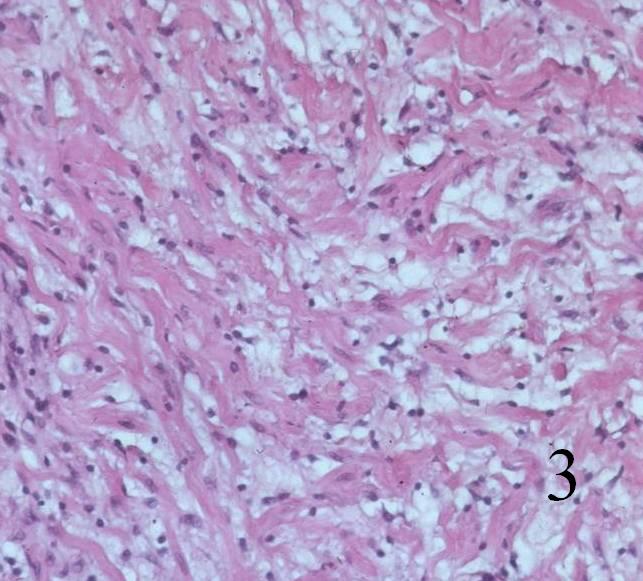 Fig. 3 Low power magnification shows wavy elongated schwann cells resembling nerve tissue
Fig. 3 Low power magnification shows wavy elongated schwann cells resembling nerve tissue
IMMUNOHISTOCHEMISTRY
•
Positive for:
o
S100 (scattered)
o
EMA
PROGNOSIS
BIOLOGICAL BEHAVIOR
•
Usually arises in small nerves in the skin
•
Readily extend into soft tissue
•
Rarely see malignant change with isolated neurofibromas
•
Low recurrence rate after surgery (even complete resection)
•
No metastasis
TREATMENT
•
Simple excision, usually adequate
•
Radiotherapy:
o
May be considered, but not usually necessary
