GENERAL INFORMATION
Angiosarcoma is a rare malignant neoplasm that arises from endothelial cells of blood vessels. Very rare in infant and young adults but has a very poor prognosis. It most typically arises in the setting of chronic lymphedema often caused by radiation and /or radical lymph node dissection for breast CANCER. Characterized by an atypical, multilayered or solid endothelial proliferation and vasoformative architecture. Can occur in the skin as well as in the deep soft tissue and very rarely as a nerve sheath neoplasm. It can also rarely arise from bone.
CLINICAL DATA
•
Early diagnosis is usually difficult
•
May be confused with a benign tumor or hematoma
•
Angiosarcomas can resemble melanoma or carcinomas histologically
•
Risk factors for developing an angiosarcoma:
• Chronic lymphedema
• Radiation
• Sun exposure
• Thorotrast
• Nodal metastases up to 14%, but also can metastases to lung, liver and bone
Differential diagnosis
•
Hemangioendothelioma
•
Hemangiopericytoma
•
Hemangioma
•
MFH
•
Pleomorphic liposarcoma
•
Hematoma
CLINICAL PRESENTATION
Signs/Symptoms
Appear cutaneously as blue-red skin lesion
Rapidly growing painless mass
Prevalence
Extremely rare, comprise a very small portion of all sarcomas
No predilection for sex or race
Occurs most often in elderly individuals and in breast cancer patients with chronic lymphedema and radiation
Sites
The skin and soft tissue angiosarcomas are most often found in the head and neck region as well as in a lymphadematous limb
May also occur in the abdominal cavity and as a nerve sheath neoplasm
Angiosarcomas may occur in the liver
RADIOGRAPHIC PRESENTATION
Plain x-ray
•
No specific radiological features (demonstrate soft tissue mass)
•
Calcifications are rare
MRI
•
Gold standard for imaging
•
Intermediate signal isointense to skeletal muscle on T1W (Fig. 1-4)
•
Heterogenous on T2W (Fig. 5-6)
•
Heterogenous enhancement after gadolinium (Fig. 3-4)
• May have significant necrosis (Fig. 3-6)
• Tumors with extensive necrosis may appear similar to a hematoma (Fig.3-4)
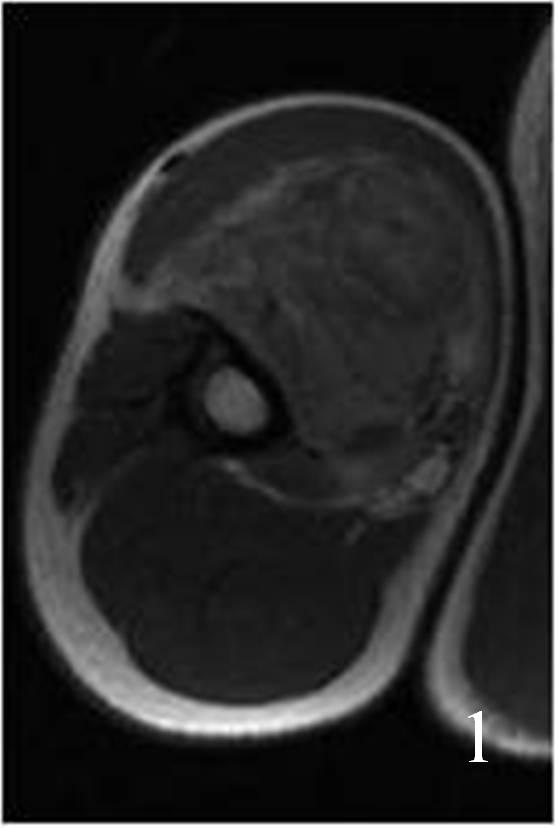
Fig. 1

Fig. 2
Fig. 1-2: Axial (Fig. 1) and coronal (Fig. 2) MRI T1W of an angiosarcoma of the arm shows a well circumscribed heterogeneous lesion. Note the high signal in the center of the mass due to hemorrhage.
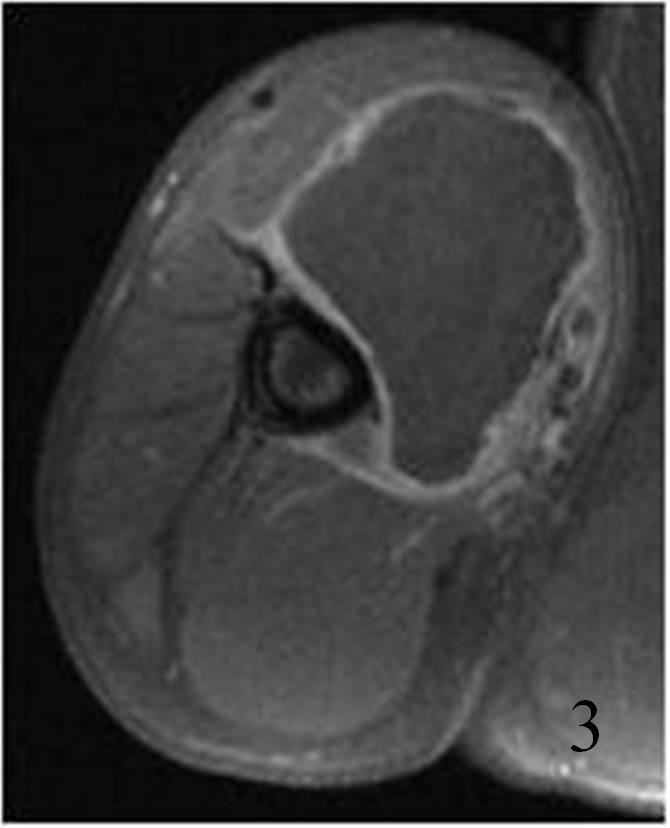
Fig. 3

Fig. 4
Fig. 3-4: Axial (Fig. 3) and coronal (Fig. 4) T1W fat suppressed and gadolinium enhanced MRI of an angiosarcoma of the arm shows a large mass that enhances almost solely around the periphery because of the extensive necrosis within the mass. There is a rim of surrounding enhancement around the mass. This can create confusion with a hematoma.
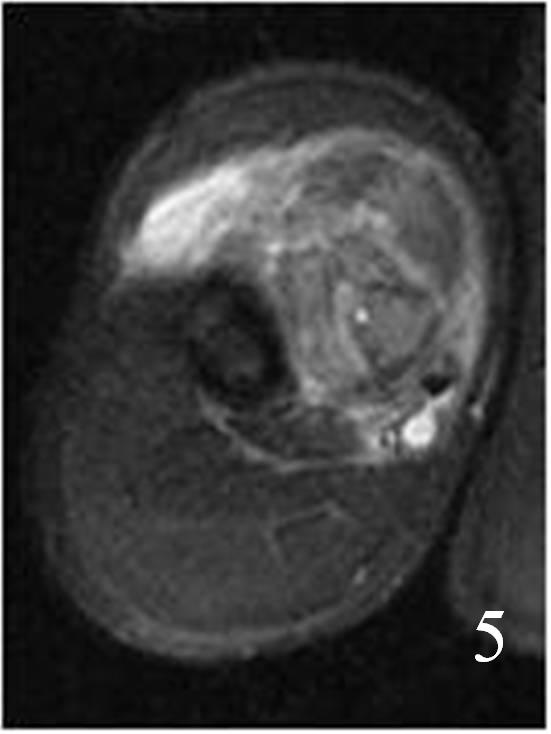
Fig. 5
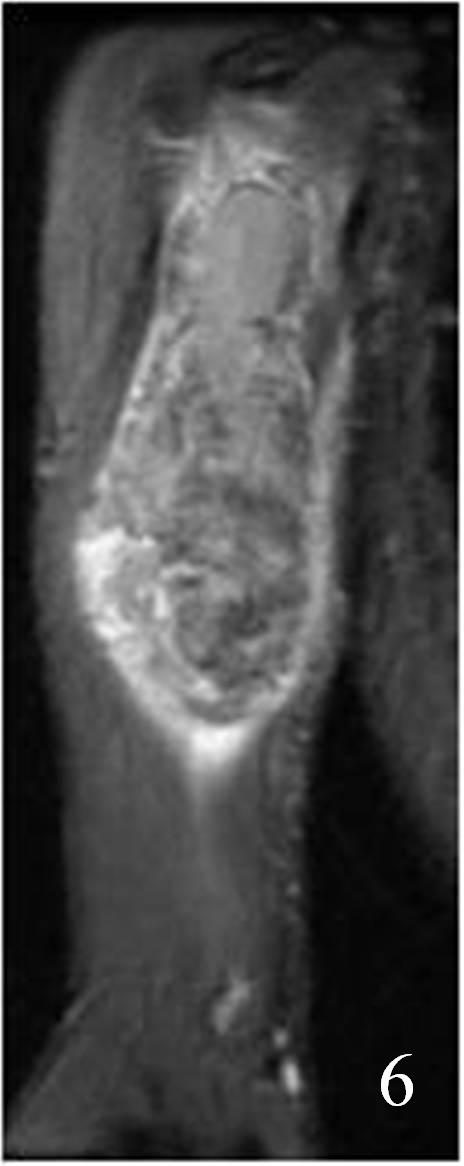
Fig. 6
Fig. 5-6: An axial (Fig. 5) and coronal (Fig. 6) T2W MRI shows a heterogeneous mass due to extensive hemorrhage and necrosis.
PATHOLOGY
Gross
•
Small, sharply demarcated, asymptomatic, multiple red nodules
or
•
Fleshy, gray-white with areas of hemorrhage and necrosis.
Microscopic
•
Well-differentiated tumors
• Characterized by entothelial cells with
• Cytologic pleomorphism
• Nuclear atypia
• Mitotic activity
• Multilayering, often with tufts or papillae
• Poorly differentiated tumors
• Endothelial cells are more atypical, close-packed, and often spindle-shaped
• Progressive loss of evident vascular channels
Immunohistochemistry
• Factor 8 related protein
• CD31
• CD34
• Ki-67
• FLI-1
• VEGFR-3 (variable)
• Keratin
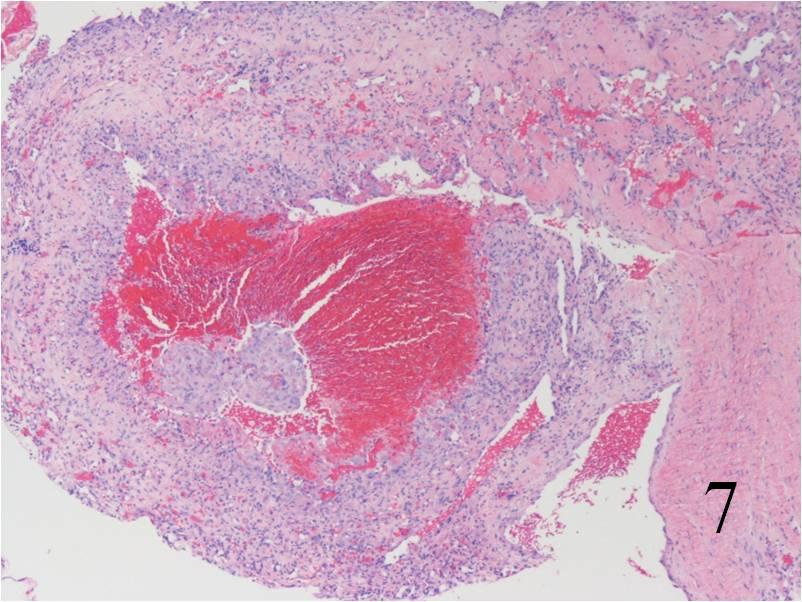 Fig. 7
Fig. 7
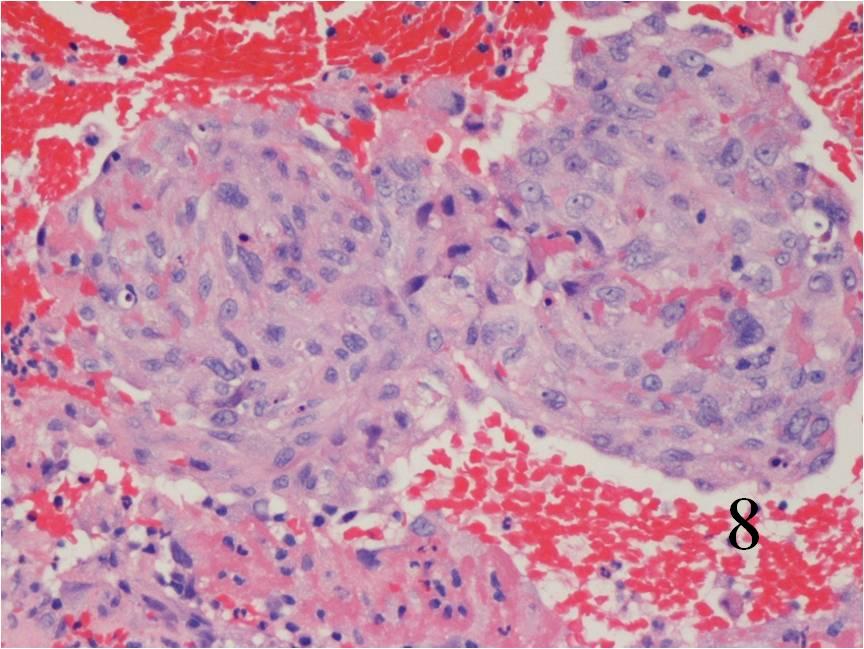 Fig. 8
Fig. 8
Fig. 7-8: Microscopic: Low (Fig. 7) and high (Fig. 8) power histology of an angiosarcoma shows abundant round to polygonal tumor cells. Fig. 8 shows nuclear atypia with mitotic activity. The cells are large with large irregular nuclei and significant pleomorphism. The cells appear somewhat epithelioid. The tumor stains positive for vimentin, Factor VIII and CD 34 (not shown in these photographs)
PROGNOSIS
Biological Behavior
• Very aggressive tumor
• Often preceded by lymphedema
• Also resulting from radiation
• Prognosis depends on several factors:
• Depth
• Size (>5 cm are associated with 5-15% survival at 5 years)
• Grade
• Lymphovascular invasion with tumor thrombi (negative prognosis)
• Tumors can be quite large, exceeding 5 cm in diameter
• Metastasis rate is high, as is the death rate
• Usual metastatic sites
• Skin and soft tissue
• Lung
• Lymph nodes
• Liver
• Bone
• There is also a tendency for satellite spreading
• Locoregional metastasis----->surgery may be ineffective
TREATMENT
• Wide and deep excision
• Positive margins are associated with high local recurrence rates
• Radiation indicated after resection; however, some patients previously treated with radiation may not be candidates for more radiotherapy
• Amputation for unresectable angiosarcomas or those that can not be resected with wide margin and are not candidates for more radiation.
• Chemotherapy (Indicated if more than 5 cm; each patient should be considered individually)
