GENERAL INFORMATION
Pleomorphic sarcoma is a high grade sarcoma of lipogenic (fatty/adipose) origin. It is a type of liposarcoma that has some lipoblasts admixed with mostly high grade pleomorphic appearing spindle cells.
CLINICAL DATA
Represents 5 to 10% of all liposarcomas
No predilection for any race or sex
Usually affecst patients between the fifth to seventh decade
Rare in younger ages
Associated with post radiation treatment in neurofibromatosis.
DIFFERENTIAL DIAGNOSIS
Plemorphic lipoma
Dedifferentiated liposarcoma
Pleomorphic rhabdmyosarcoma
Undifferentiated pleomorphic sarcoma
CLINICAL PRESENTATION
Signs/Symptoms
Large mass
Slowly growing tumor
Usually painless
Prevalence
No predilection for any sex or race
Less than 10% of all soft tissue sarcomas
Site
Does not have a strong locational predilection
Most commonly intramuscular or in other deep sites
Occasionally occurs in subcutaneous tissue
RADIOGRAPHIC PRESENTATION
Plain x-ray
No specific radiological features
May reveal a soft tissue mass
CT
Often heterogenous with density similar to muscle
MRI
Large mass with heterogeneous signal intensity (Fig. 1, 2)
Strong enhancement post gadolinium (suggestive of malignant process)
Areas of necrosis and hemorrhage
Usually it is very difficult to detect any fat within the mass on an MRI
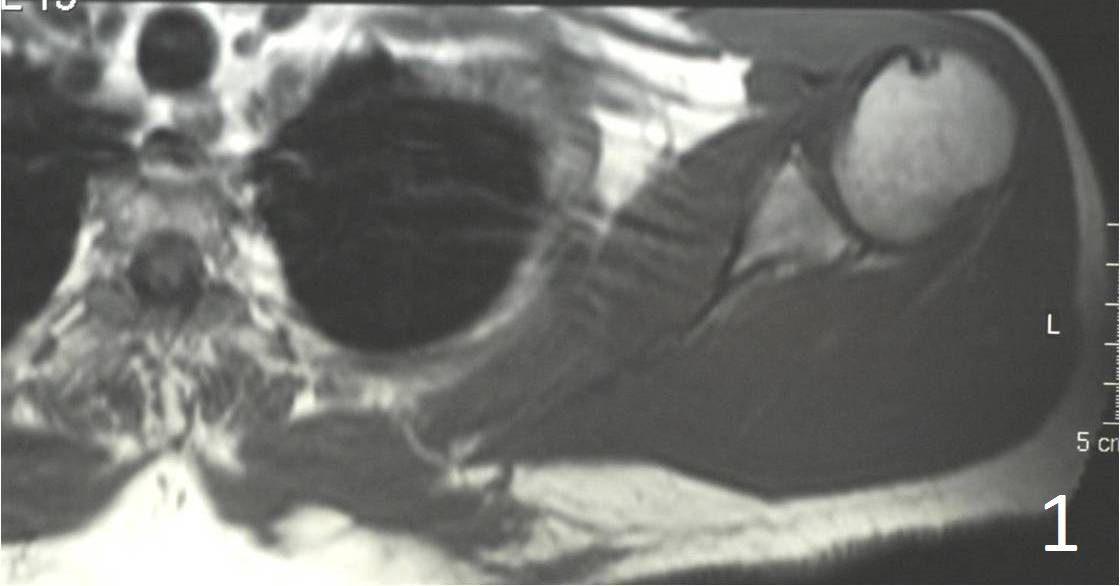
 Fig. 1, 2 Axial MRI of shoulder shows a lesion in the subcutaneous tissue along the postermedial border of the scapula.
Fig. 1, 2 Axial MRI of shoulder shows a lesion in the subcutaneous tissue along the postermedial border of the scapula.
PATHOLOGY
Gross
Often large (8-10 cm), may up to 20 cm; multiodular (Fig. 3)
Areas of hemorrhage and necrosis common
Usually has a sarcomatous fleshy appearance
Sometimes has partly or wholly myxoid component
May contain white-yellow coloration
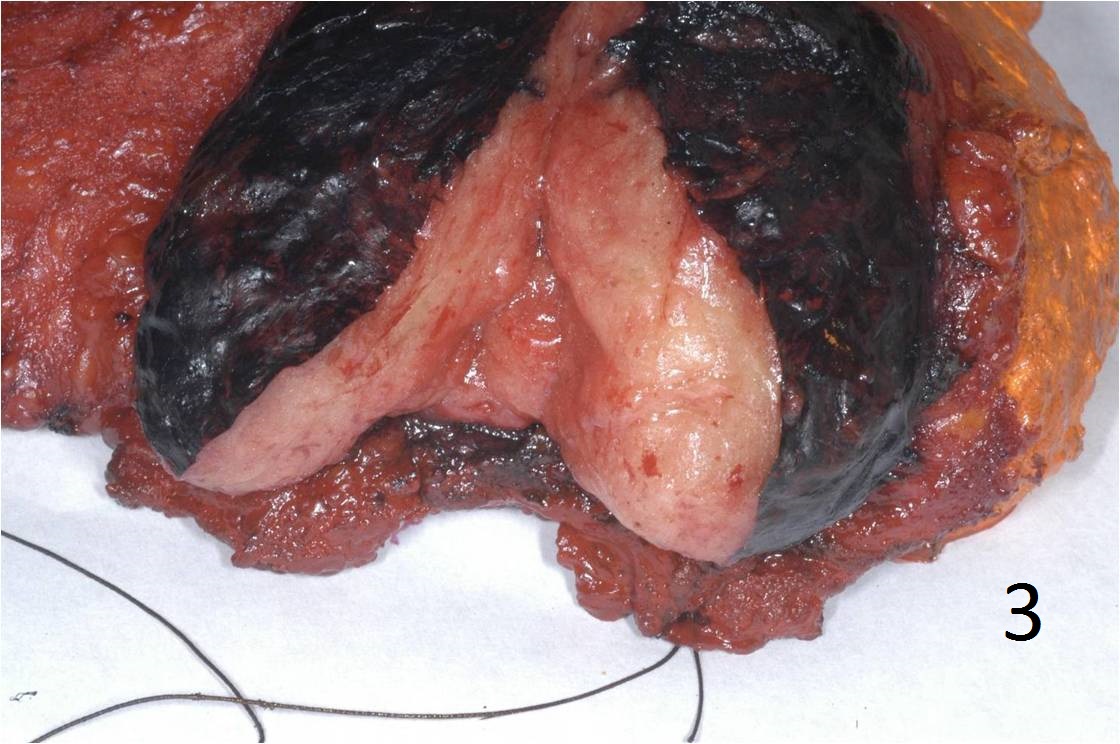 Fig. 3 Gross Pathology: Photo of a gross specimen.
Fig. 3 Gross Pathology: Photo of a gross specimen.
Microscopic
Well circumscribed, but non-encapsulated
Cellular in nature
Tumor necrosis common
Moderately to markedly pleomorphic (Fig. 4 and 5)
Myxoid areas
Less cellular
Retain pleomorphism
Tumor cells:
Large cells and cytologically malignant
Nuclei are elongate, round or bizarre
Mitosis 10 high per field
Commonly multinucleated
Some contain identifiable lipid vacuoles
Sharply outlined
Appear empty
Indent the nucleus
No mature fat cells
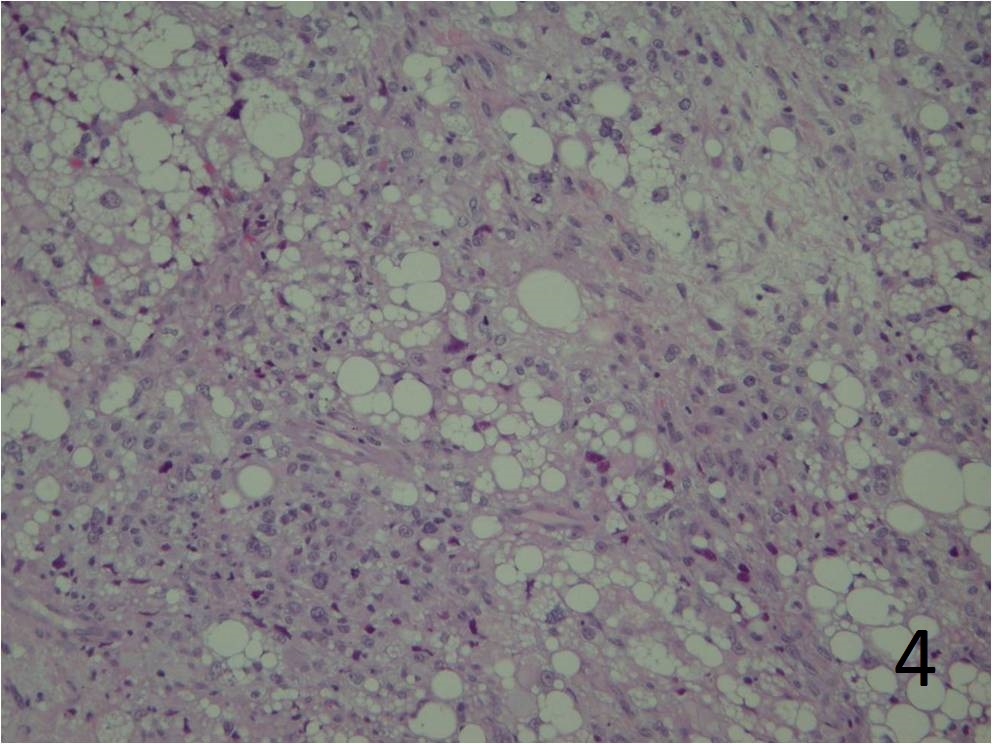
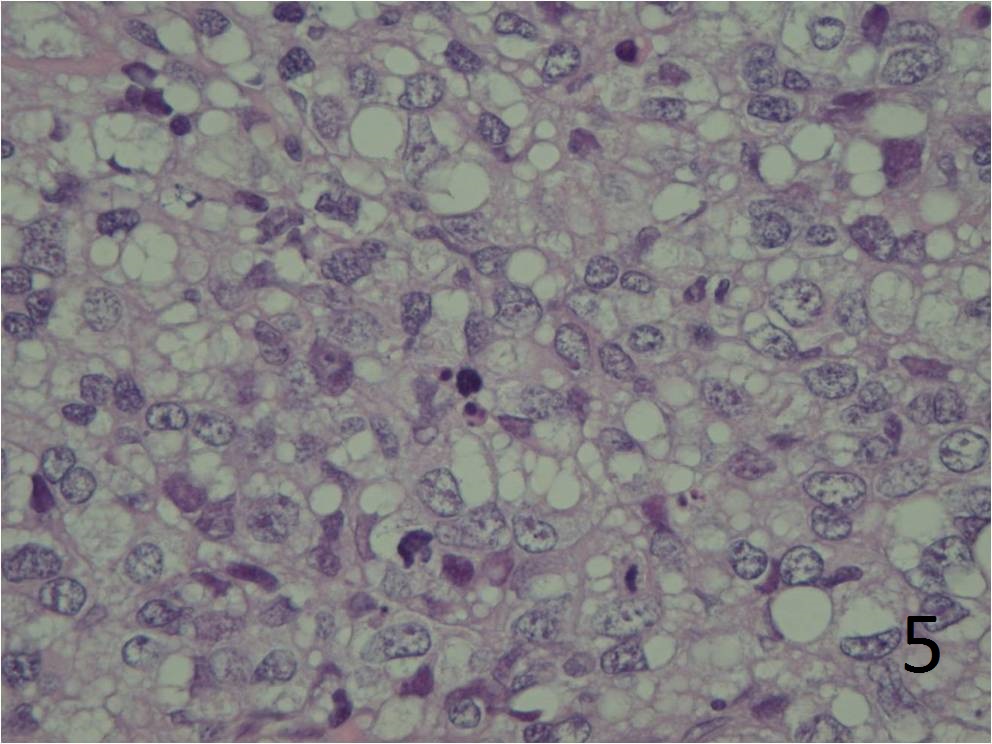 Fig. 4 Microscopic: Intermediate and high (Fig. 5) power magnification show prominent pleomorphism, and many lipid vacuoles; cells are large and multinucleated. The lipoblasts are pleomorphic.
Fig. 4 Microscopic: Intermediate and high (Fig. 5) power magnification show prominent pleomorphism, and many lipid vacuoles; cells are large and multinucleated. The lipoblasts are pleomorphic.
IMMUNOHISTOCHEMISTRY
Vimentin
S100
Smooth muscle actin
CD34
Keratin
Desmin
PROGNOSIS
Biological Behavior
High risk for local recurrence (wide excision option for treatment)
High risk for metastasis
Less than 60% survival over 5 years
Poor prognostic factors:
˃60 yo
Truncal location
Deep to fascia
Larger than 5 cm
Vascular invasion
Incomplete excision
TREATMENT
Wide excision (Fig. 6 and 7)
Radiotherapy and chemotherapy
Chemotherapy may be controversial
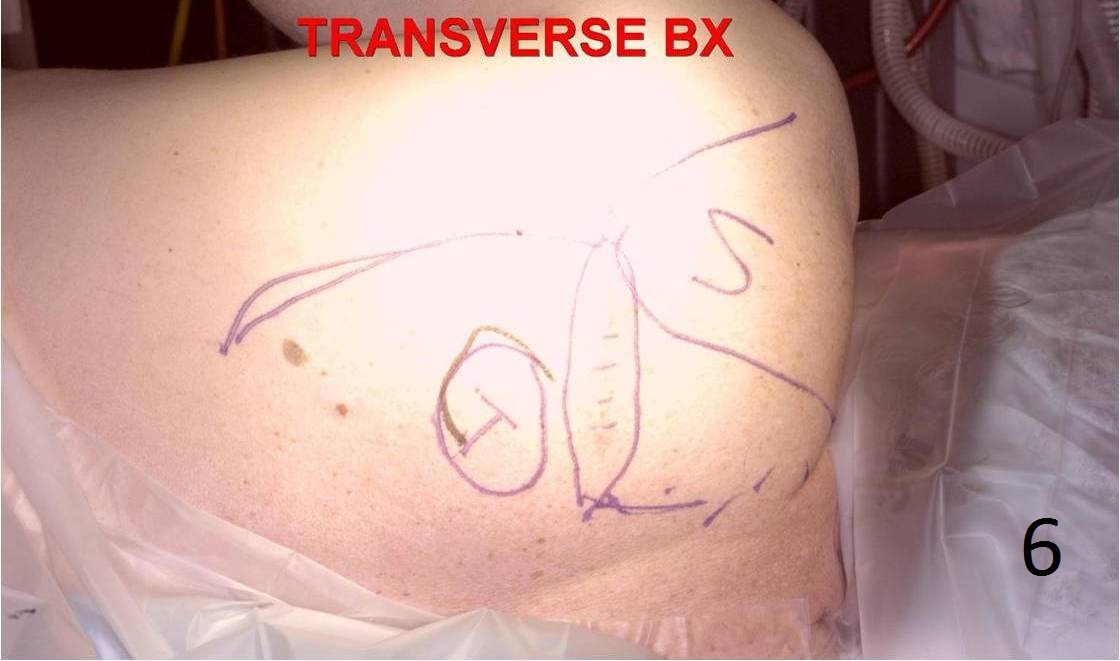 Fig. 6 Intraoperative photograph of skin incisions to remove a pleomorphic liposarcoma from the trapezius area. The patient had a previous biopsy through a transverse incision. Transverse incisions should rarely be used to biopsy a tumor.
Fig. 6 Intraoperative photograph of skin incisions to remove a pleomorphic liposarcoma from the trapezius area. The patient had a previous biopsy through a transverse incision. Transverse incisions should rarely be used to biopsy a tumor.
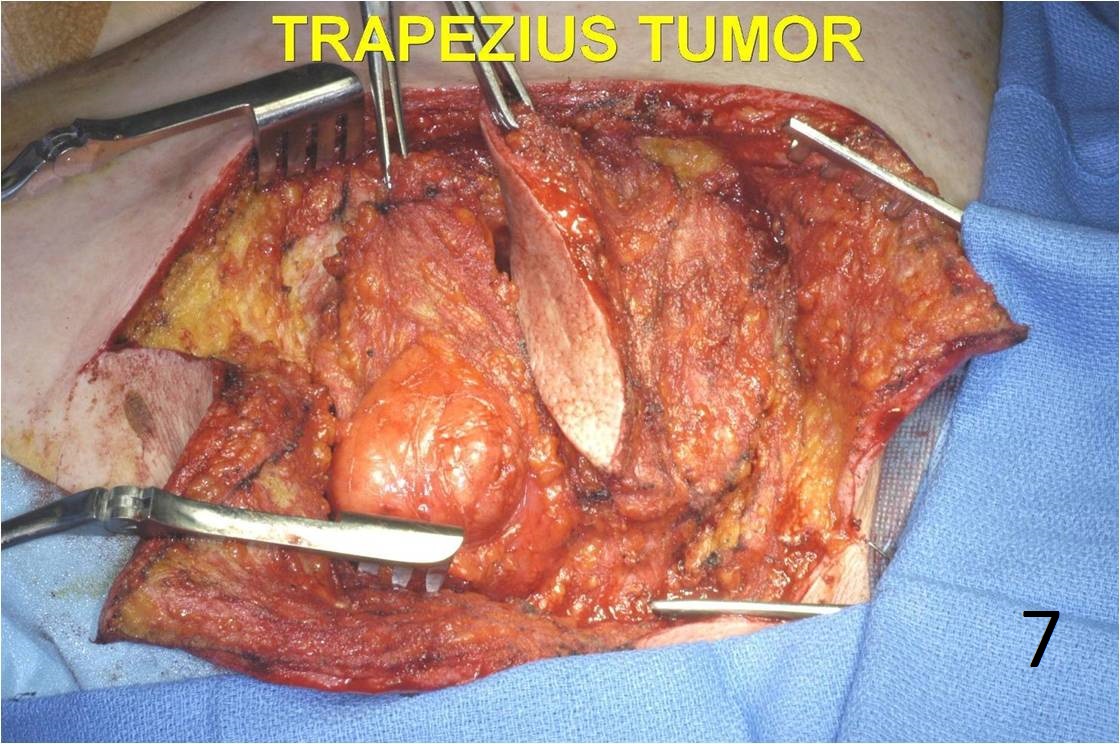 Fig. 7 Photograph shows the tumor and the biopsy tract.
Fig. 7 Photograph shows the tumor and the biopsy tract.
