GENERAL INFORMATION
A fibrosarcoma is a malignant (cancerous) spindle cell neoplasm originating from fibroblasts that shows no other evidence of differentiation. The spindle cells are usually uniform and show minimal pleomorphism depending on the grade of the tumor. Fibrosarcoma usually arise in the soft tissue, though can rarely arise in bone. They are often categorized according to grade, as Grade 1, 2 or 3.
CLINICAL DATA
• Affects all ages
• Most common between ages 30-55
• Slow growing and usually painless
• Presents pain in 30% of cases
• May arise secondarily:
• Irradiated soft tissue
• Scars and burns
• Dedifferentiated component of Dermatofibrosarcoma Protuberans (DFSP)
• Dedifferentiated component of liposarcoma
• Sites:
• Most common in thigh, leg and pelvis
• May also occur in trunk/upper extremity
Differential diagnosis
Other soft tissue sarcomas:
• Dedifferentiated liposarcoma
• Malignant fibrous histiocytoma (now known as undifferentiated pleomorphic sarcoma; In past also known as a Grade 3 fibrosarcoma)
• Dedifferentiated liposarcoma
• Synovial sarcoma: monophasic
• Leiomyosarcoma
• Malignant peripheral nerve sheath tumor (MPNST)
CLINICAL PRESENTATION
Signs/Symptoms
• Solitary palpable mass
• Mean 3-8 cm in diameter
• Slow-growing mass
• Usually painless mass (presents with pain in 1/3 of cases)
Prevalence
• Slight predilection towards males
• 5% of all soft tissue sarcomas
• Not very common (many tumors formerly classified as fibrosarcoma, have been redefined as another entity because og special immunohistochemical stains)
• Can affect all ages, but more common between third and fifth decade.
• Infantile form in <10 years of age
Sites
• Intramuscular, rarely in subcutaneous tissue
• Affects:
• Arm/ shoulder girdle
• Forearm
• Trunk
• Buttock, thigh, knee, legs (more common affected areas)
RADIOGRAPHIC PRESENTATION
Plain x-ray
• No specific radiological features
• Soft tissue density.
• May be evidence of bone deformity/erosion, secondary to bone destruction
CT
• Good for detecting bone involvement (Fig. 1)
• Isointense to muscle
MRI
• 60% of fibrosarcomas are intramuscular (Fig. 2, 3, 5, 6, 7, 8)
• Well defined heterogenous mass on T2W (Fig. 4, 9)
• Necrosis and hemorrhage are common, especially in high grade tumors
• On gadolinium, viable areas of tumor enhance, while areas of significant necrosis and hemorrhage do not enhance (Fig. 6).
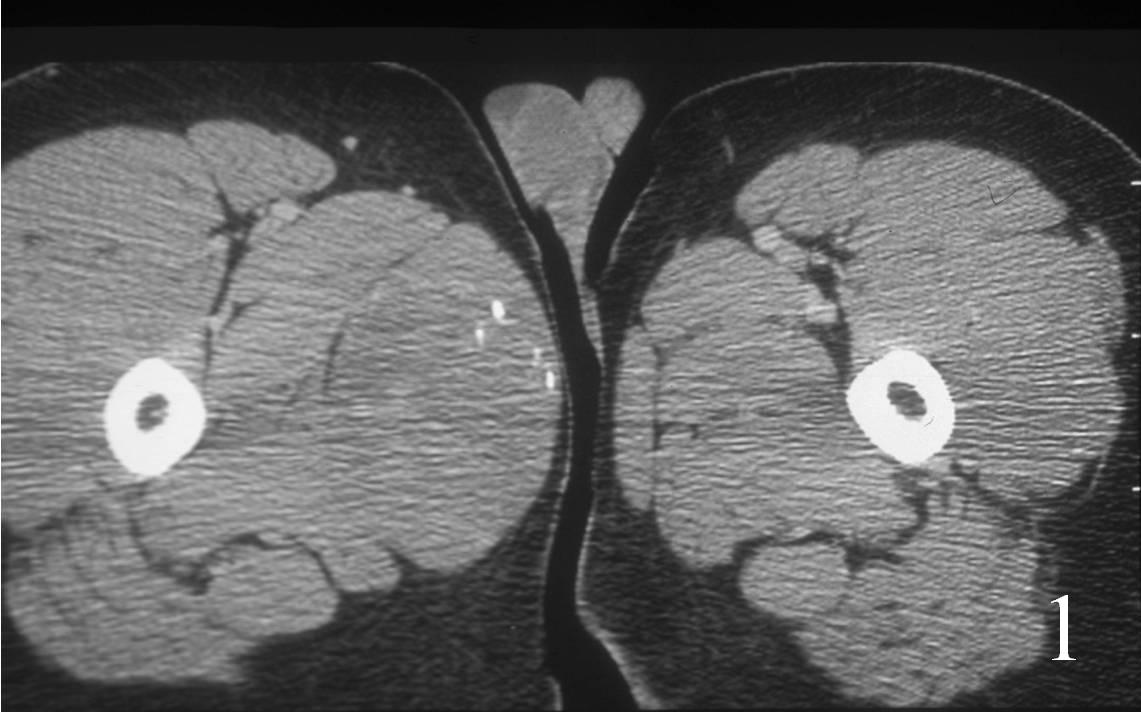 Fig. 1: Axial CT reconstruction of thigh demonstrates an isointense mass in the vastus medialis consistent with a fibrosarcoma
Fig. 1: Axial CT reconstruction of thigh demonstrates an isointense mass in the vastus medialis consistent with a fibrosarcoma
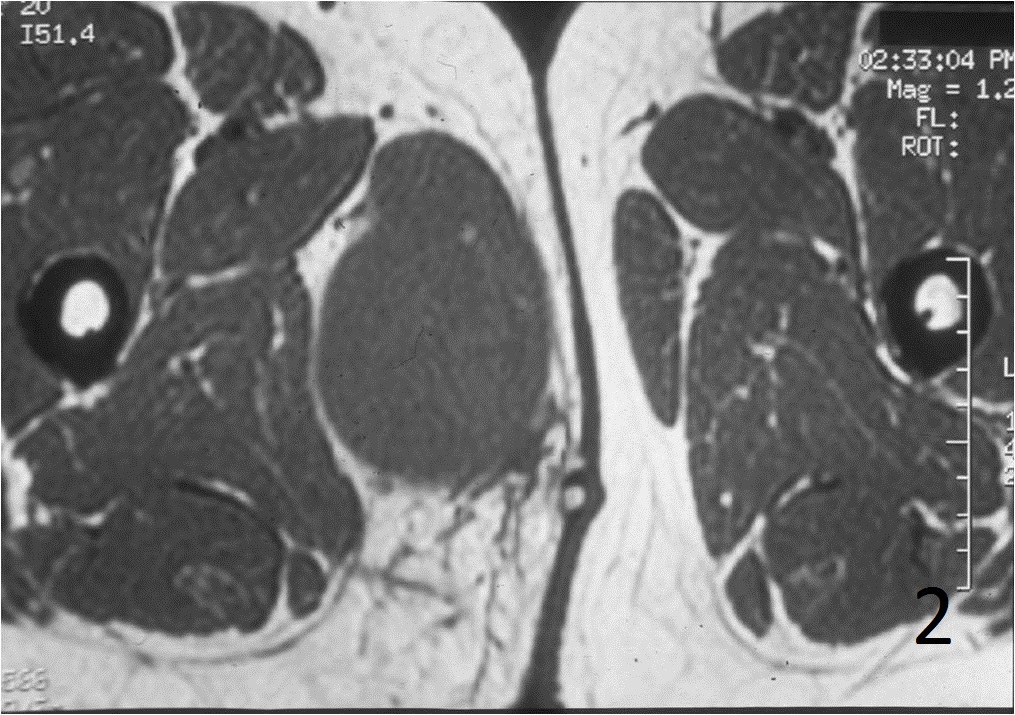
Fig. 2
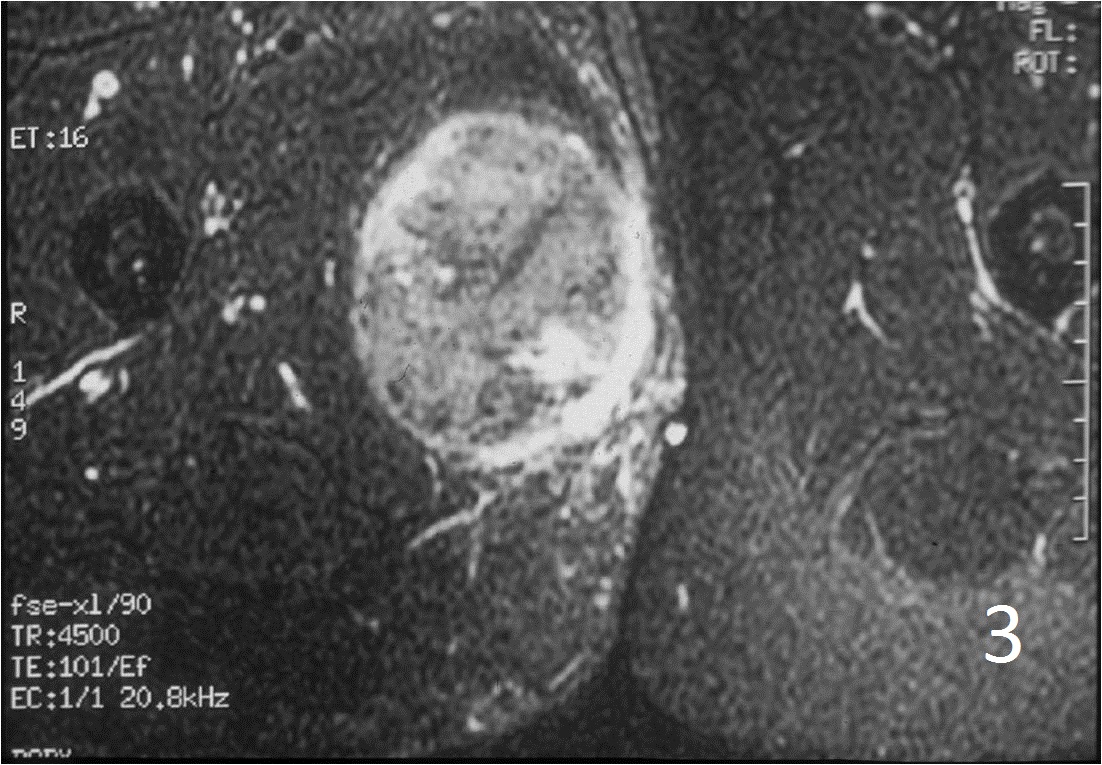
Fig. 3
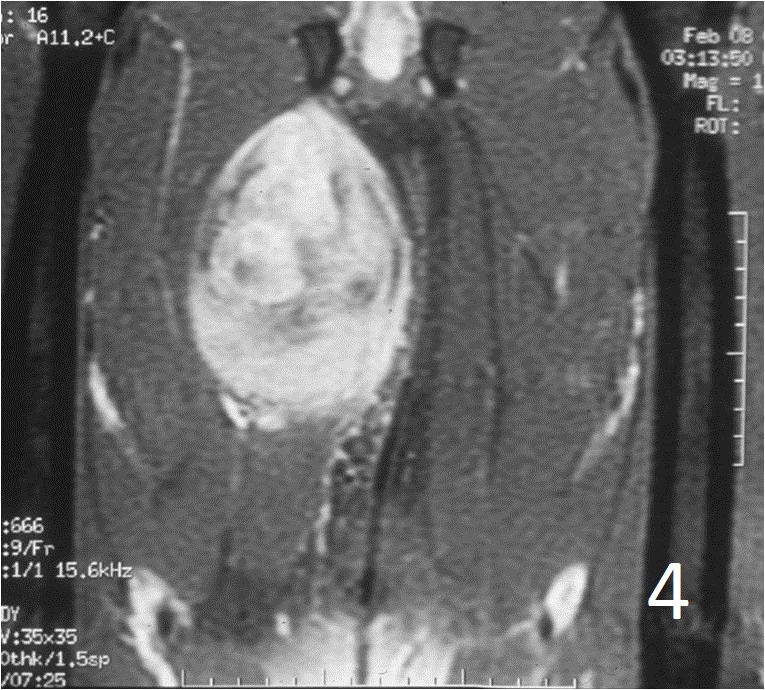
Fig. 4
Fig. 2-4: An MRI of the thigh shows a mass in the medial compartment that is isointense to muscle on T1W images (Fig. 2) and heterogeneous on T2W (Fig. 3). Sagittal T1W post contrast with gadolinium demonstrates enhancement of the tumor (Fig. 4).
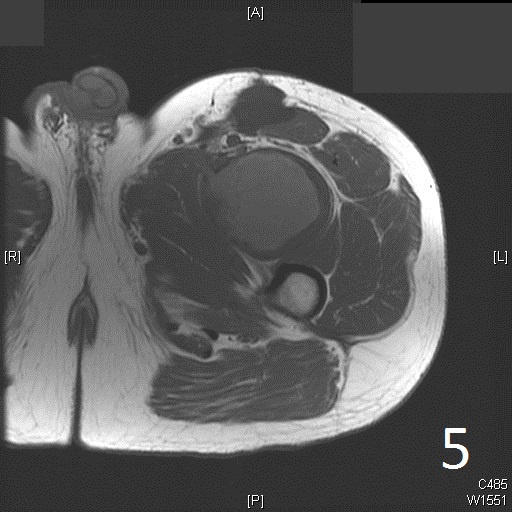
Fig. 5
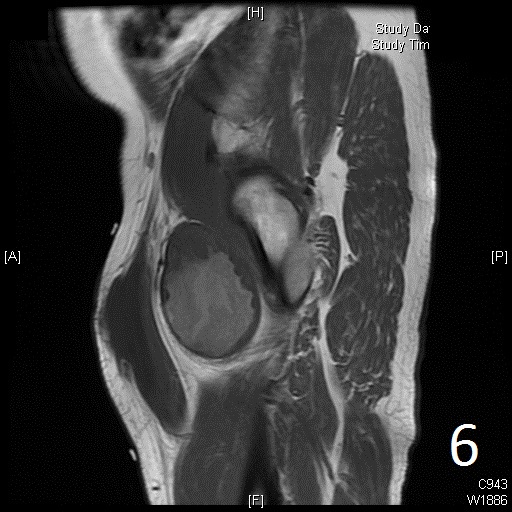
Fig. 6

Fig. 7
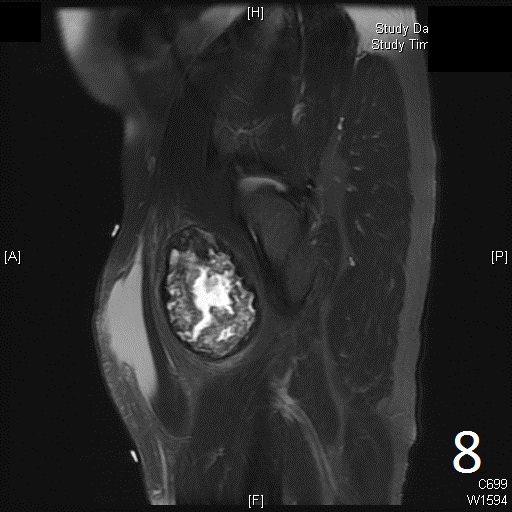
Fig. 8
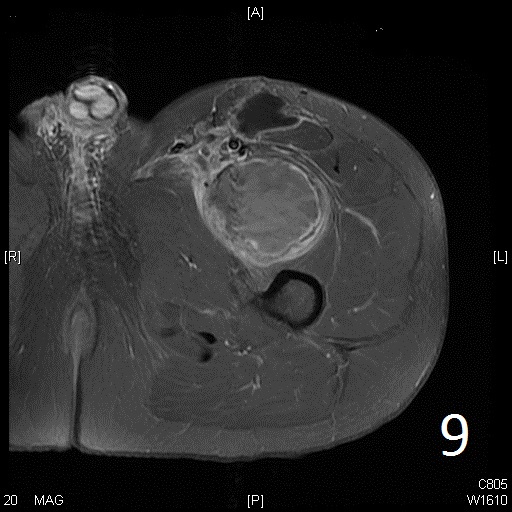
Fig. 9
Fig. 5-9: Axial and sagittal (Fig. 6) MRI shows a fibrosarcoma in the proximal quadriceps muscle that is isointense to muscle on T1W images, and a heterogeneous on T2W FS (Fig. 7, 8). The patient was treated with preoperative chemotherapy and the mass underwent extensive necrosis. The mass does not show any enhancement with contrast due to the extensive necrosis. There is only peripheral enhancement with contrast on T1W FS (Fig. 9).
PATHOLOGY
Gross
•
Fleshy, focally necrotic and hemorrhagic mass--->High grade (Grade 2-3) tumors (Fig. 10)
• Firm and rubbery mass, like fibromatosis----->low grade (Grade 1), well differentiated, collagenized.
Microscopic
•
Elongated, fairly uniform spindle cells with scant cytoplasm in a fibrous stroma
• Large nuclei with abnormal mitoses present; Higher grade tumors have more mitoses, necrosis and pleomorphism.
• Minimal pleomorphism with low grade tumors; More pleomorphism and mitoses with higher grade tumors
• Herringbone pattern (fascicles that intersect at right angles) (Fig. 11)
• Nuclei appear elongated with round ends (Fig. 12)
Immunohistochemistry
• Vimentin positive; Keratin negative
• Actin variable; perhaps minor scant staining
• S-100 negative
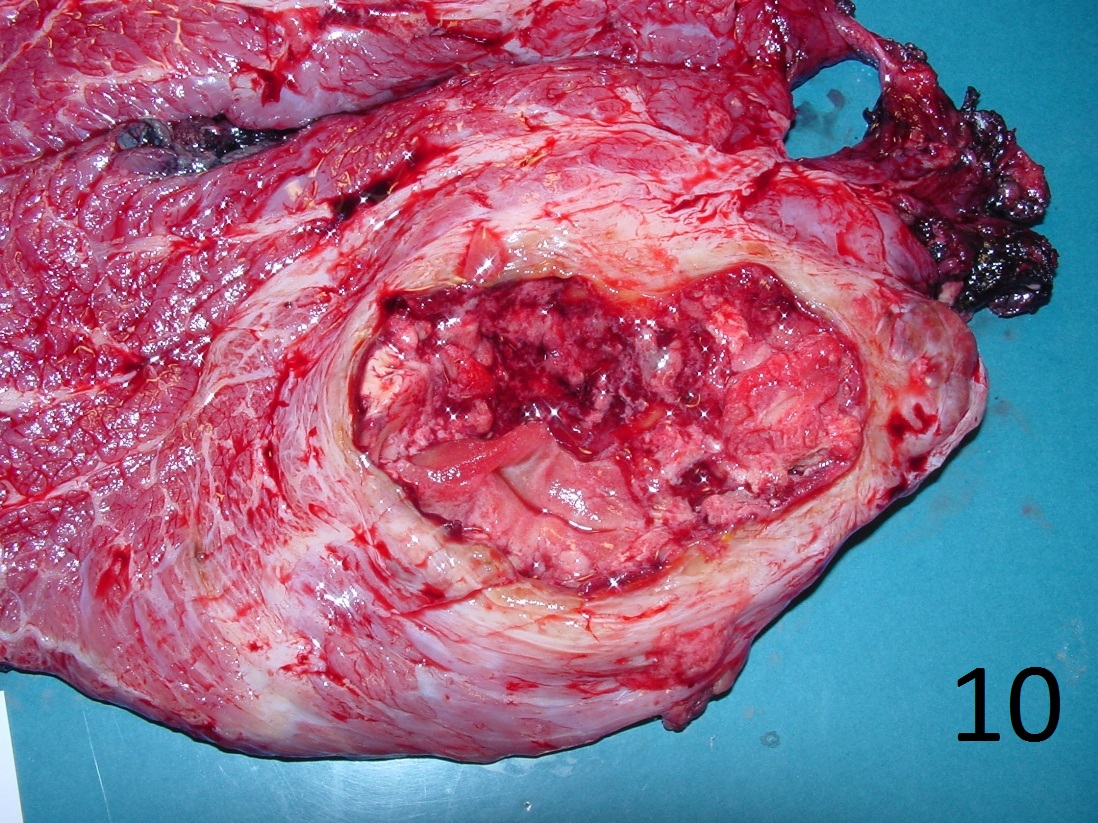
Fig. 10: Photograph of gross specimen of fibrosarcoma of buttock after radical resection
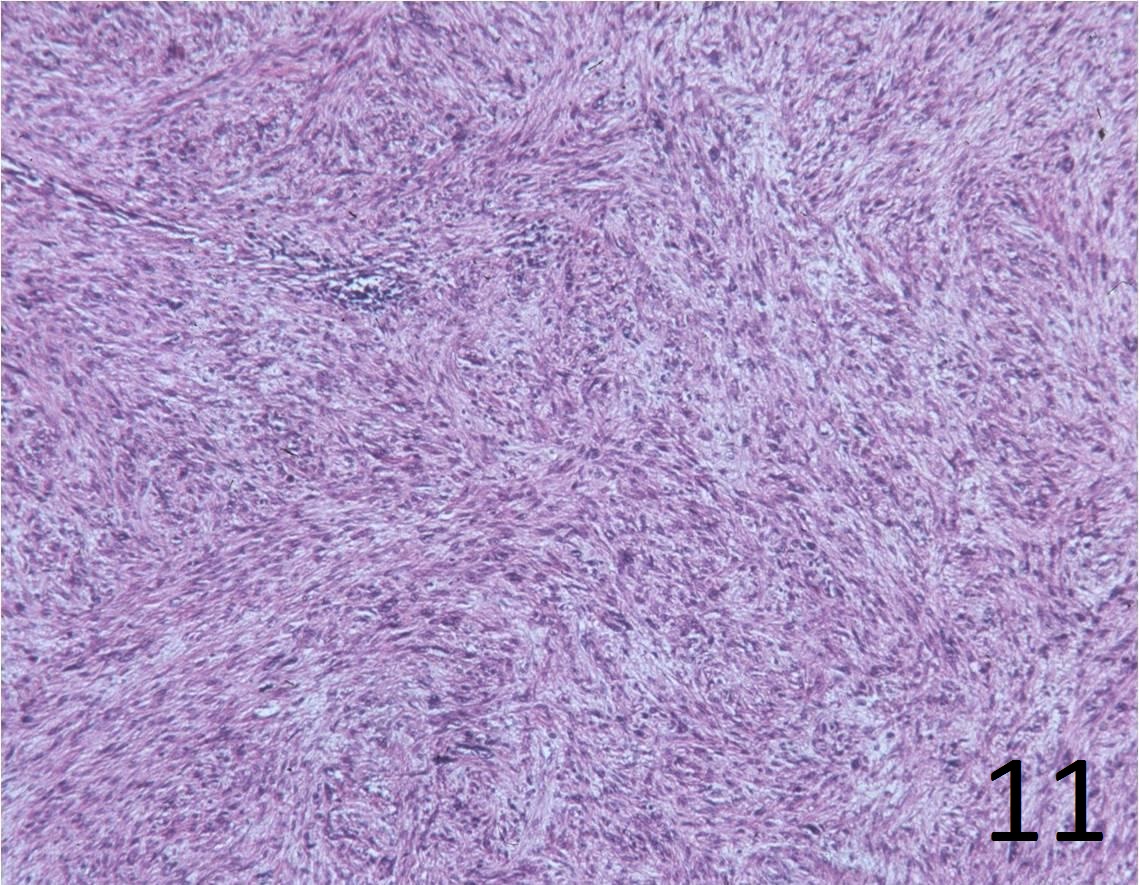
Fig. 11: Microscopic: Low power magnification H&E shows a spindle cell sarcoma with a typical herringbone pattern.
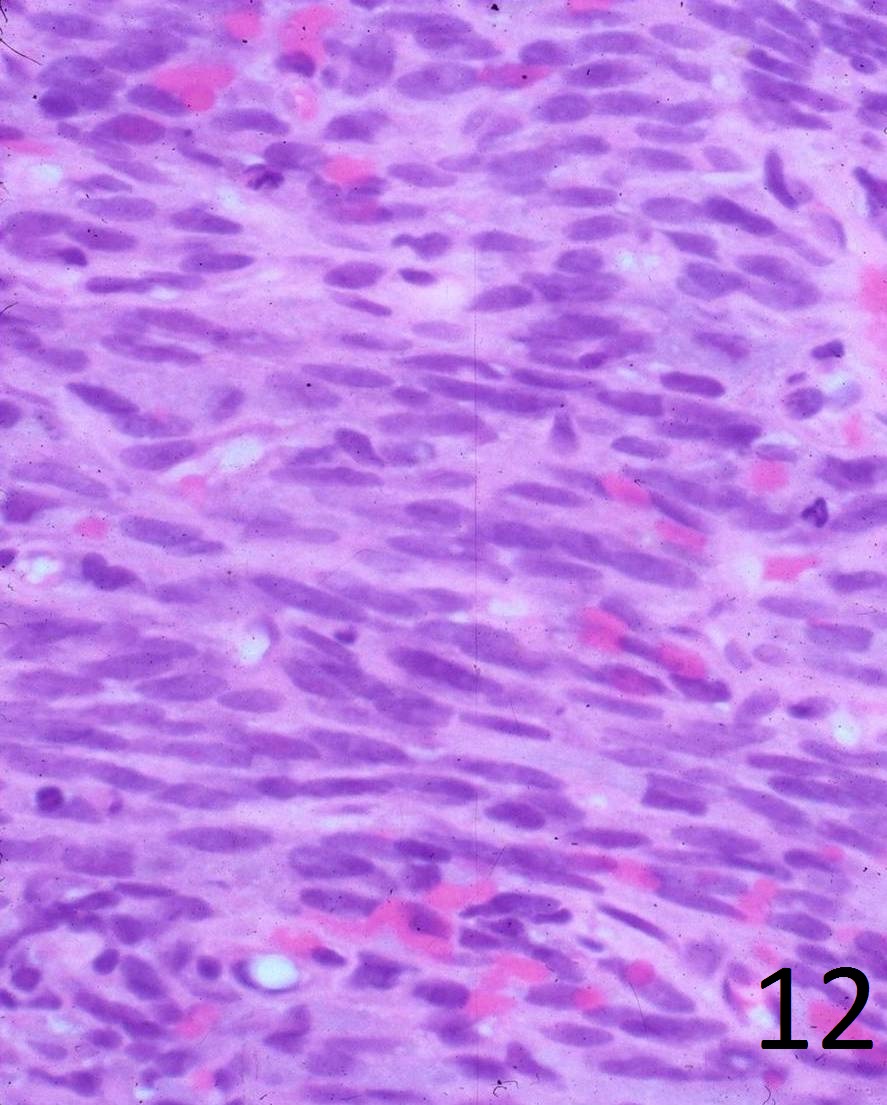
Fig. 12: High power magnification shows elongated spindle cells (cigar shaped cells) with large nuclei, scant cytoplasm and frank pleomorphism. There are abnormal mitoses and there is a fibrous tissue matrix interspersed between the cells. The cells are producing fibrous tissue.
PROGNOSIS
Biological Behavior
• Fibrosarcomas in childhood metastasize in fewer than 10% of cases
• Overall 5-year survival is 40-60% in adults
• More than 60% metastasize (lung, bone, liver)
• Prognosis is related to grade, size and location of the tumor:
• Grade 1: Rarely metastasize (approximately 10%)
• Grade 2-3: 35-45% chance of metastases
TREATMENT
• Wide resection +/- radiation (Fig. 13,14,15)
• Amputation for unresectable cases
• Chemotherapy may be indicated for certain patients
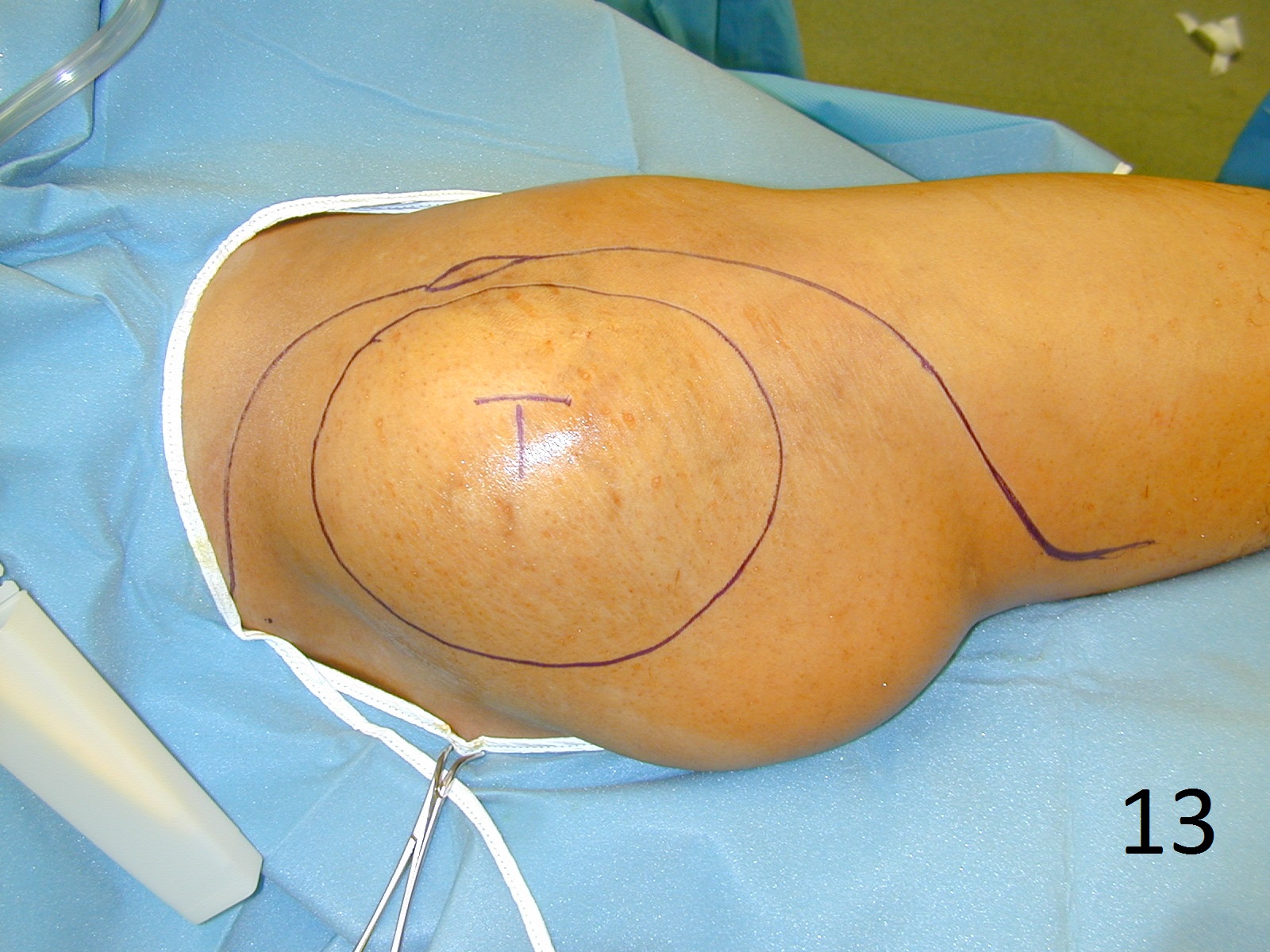
Fig. 13

Fig. 14
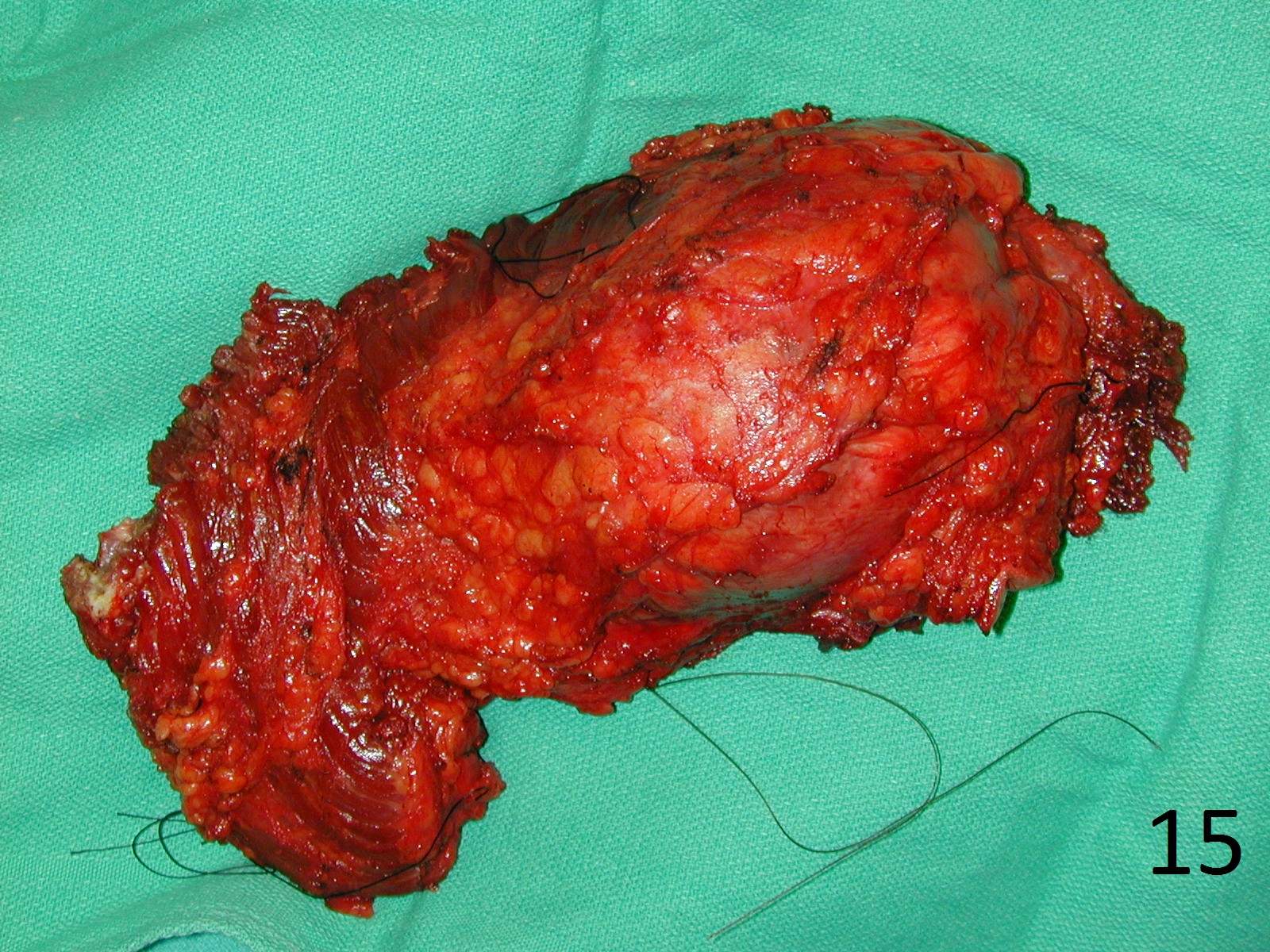
Fig. 15
Fig. 13-15: Intraoperative photograph of a radical resection of fibrosarcoma of the buttock (Gluteus Maximus Muscle) (Fig. 13,14,15).
