GENERAL INFORMATION
Tumoral calcinosis is a very rare entity, characterized by large tumorlike calcium deposits and painless mass, arising near to the articular soft tissue areas. Common areas affected are elbows, hips, knees rarely involve hands and feet. No obvious metabolic calcium deficiency or disorder.
Multiple lesions may affect 2 or more siblings or generations in a family.
CLINICAL DATA
• History of:
• Injury
• Renal failure
• Endocrine problem
• Hyperthyroidism
• Hyperparathyroidism
• Myeloma
• Sarcoidosis
•
Rarely is familiar
•
Lab:
• Elevated calcium
• Elevated phosphate
• Elevated vitamin D
Differential diagnosis
• Dystrophic calcification
• Extraskeletal Osteosarcoma
• Heterotopic Ossification
• Myositis Ossificans
• Heavily Ossified Synovial Sarcoma
CLINICAL PRESENTATION
Signs/Symptoms
• May cause local pain and tenderness
• Mild to moderate hypercalcemia and hyperphosphatemia
Prevalence
• Children and young adults
• Afro-American heritage
• First to third decade of life
Sites
• Calcifications located in the periarticular soft tissue areas near to major joints
• Hips, shoulders, elbows, knees, rare in hands and feet
• Frequent bilateral symmetry
RADIOGRAPHIC PRESENTATION
Plain x-ray (Fig. 1-2)
• Reveal well defined opacities in soft tissue
• Foci of calcification are few millimeters to 2 cm of size
• Lobulated calcifications separated from the bone
MRI
• Cystic changes fluid level may be seen
• Ossification is low signal on T1 and T2 W images
 Fig. 1
Fig. 1
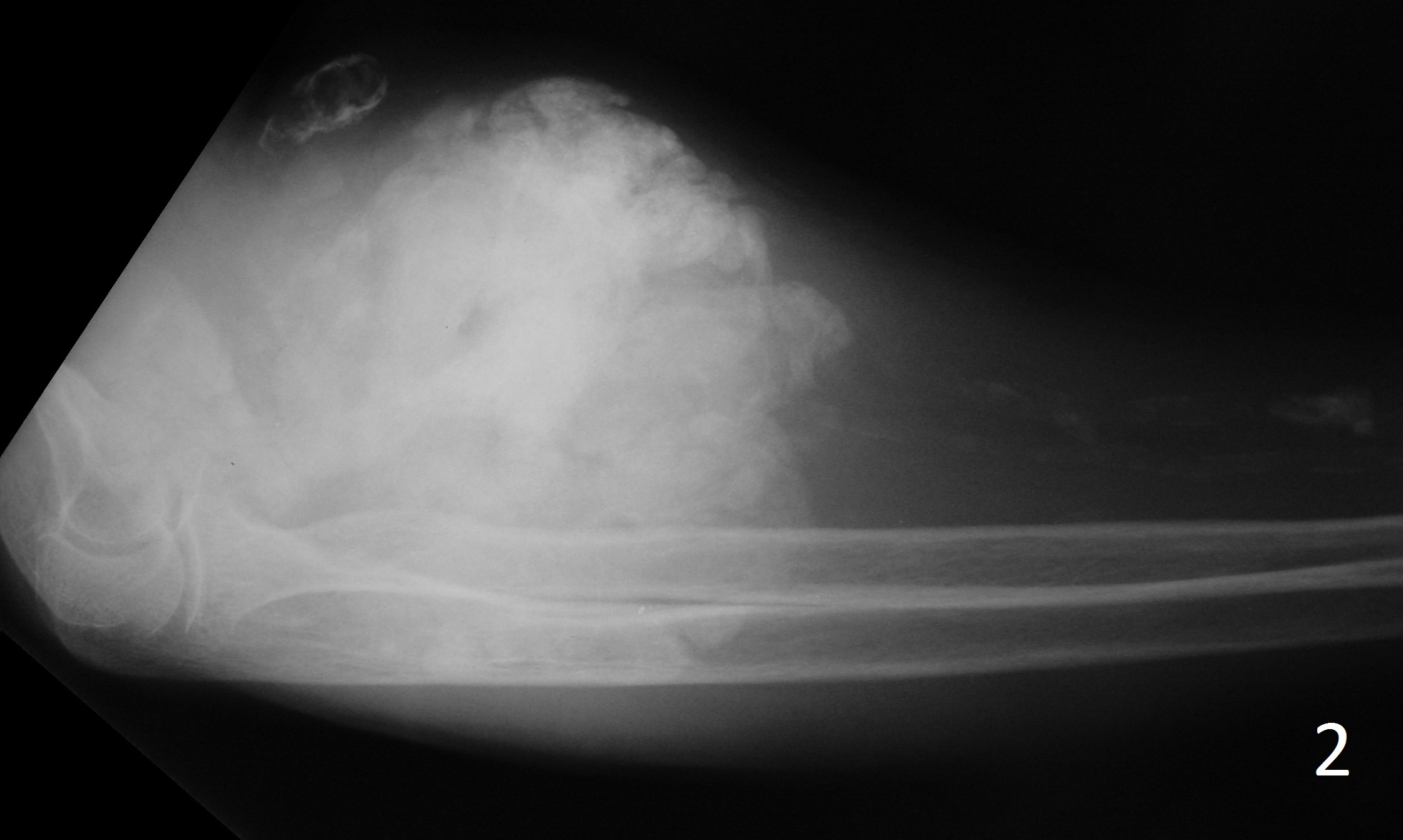 Fig. 2
Fig. 2
Fig. 1-2: AP (Fig. 1)and lateral (Fig. 2) xray of elbow show exuberant ossification around the elbow joint consistent with tumoral calcinosis in this patient with chronic renal failure.
PATHOLOGY
Gross
•
Firm encapsulated chalky mass consisting of many calcified nodules
• Nodules focally coalesce into larger masses
• Nodules filled with yellow/grey, past or milky fluid
Microscopic
•
Nodules have large areas of amorphous or granular calcium masses
• May have interspersed calcopherites
• Calcium crystals exhibit hydroxyapatite
• Macrophage infiltration, osteoclast-like giant cells, inflammatory cells present
PROGNOSIS
Biological Behavior
• Incompletely excised lesion exhibit recurrence
• Lesion lasting long term may develop infection and abscess formation
• Similar calcification may be present in patient with calcium disorder
• Renal disease or secondary hyperparathyroidism
TREATMENT
• Surgical excision is most popular treatment when symptomatic
• Calcium deprivation and PO4 binding antacid have been used as alternative therapy
• Radiotherapy, cortisone, aluminum hydroxide gels are not effective
