GENERAL INFORMATION
Malignant peripheral nerve sheath tumor (MPNST) is a malignant form of the schwannoma. It is a spindle cell sarcoma that can arise from a neurofibroma and shows nerve sheath differentiation.
CLINICAL DATA
- Associated with neurofibromatosis 1 (NF1) (25-70%)
- Is found in younger patients when associated with NF1 (20-70%)
- High grade sarcoma
- Suspect in sudden enlargement of neurofibroma
- Can be associated with post radiation treatment
- Commonly spreads when epineurium/perineurium is involved
- Associated with rhabdomyosarcoma components (Triton tumor)
DIFFERENTIAL DIAGNOSIS
CLINICAL PRESENTATION
Signs/Symptoms
- Pain is common
- Slowly growing tumor
- Occasionally there may be neurological symptoms
Prevalence
- No predilection for any sex or race
- 10% of all soft tissue sarcomas
- Occurs in all ages
- Associated with neurofibromatosis 1 (25-70%) (Fig. 1)
- Preference for individuals between 20 and 50 years of age
 Fig. 1 Clinicial photograph of patient with Neurofibromatosis 1 showing dermal neurofibromas and cafe au lait spots
Fig. 1 Clinicial photograph of patient with Neurofibromatosis 1 showing dermal neurofibromas and cafe au lait spots
Site
- Most commonly associated with major nerve trunks
- Often found on the proximal aspects of the upper extremities and trunk
- Very rarely found in the head/neck
RADIOGRAPHIC PRESENTATION
Plain x-ray
- No specific radiological features
- May reveal a soft tissue mass
- Mature areas of osteoid or chondroid mineralization may occur
- Displacement of neurovascular bundle may also be apparent
CT
- High attenuation rim
- Hypointense mass
MRI
- MPNST, Schwannoma, and neurofibroma may be indistinguishable radiologically
- MPNST usually presents as large mass (5 cm) with fusiform shape
- Increased vascularity at proximal-distal pole of the lesion (corkscrew vessels)
- No well defined margins of the tumor, infiltrative pattern.
- Heterogeneous areas
- Isointense to higher signal than muscle on T1W (Fig. 2, 3)
- High signal intensity on T2W
- With gadolinium (Fig. 4, 5)
- Reverse target post-contrast
- Increased gadolinium uptake------->unlike peripheral nerve sheath tumor (PNST)
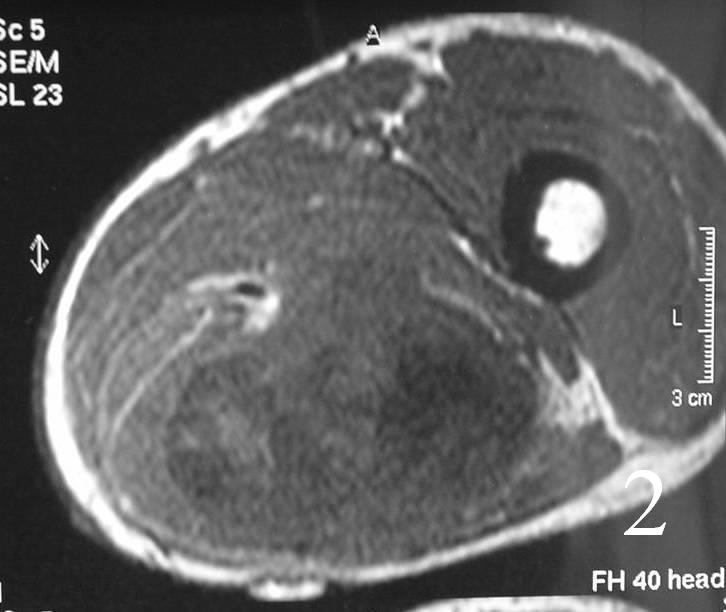
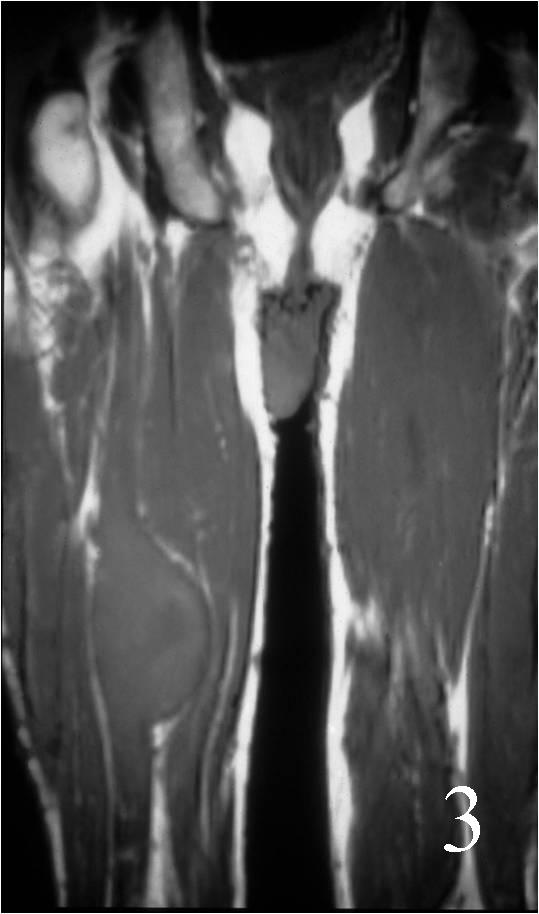
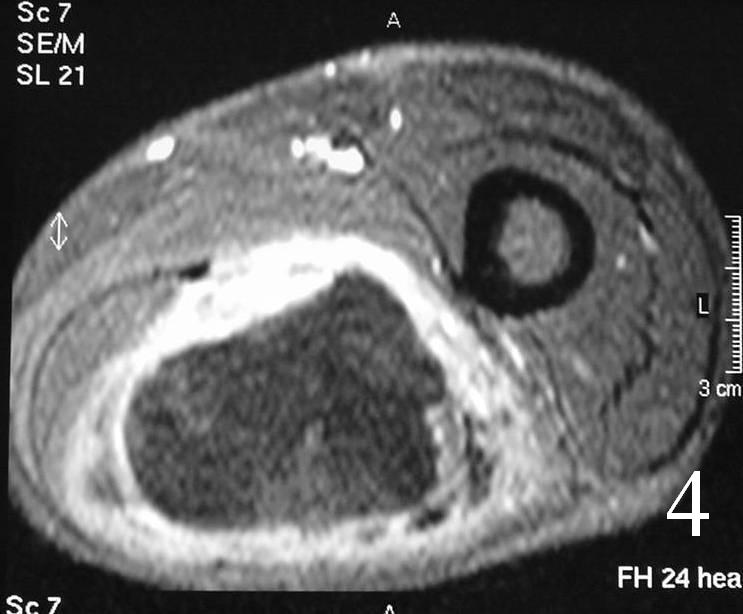
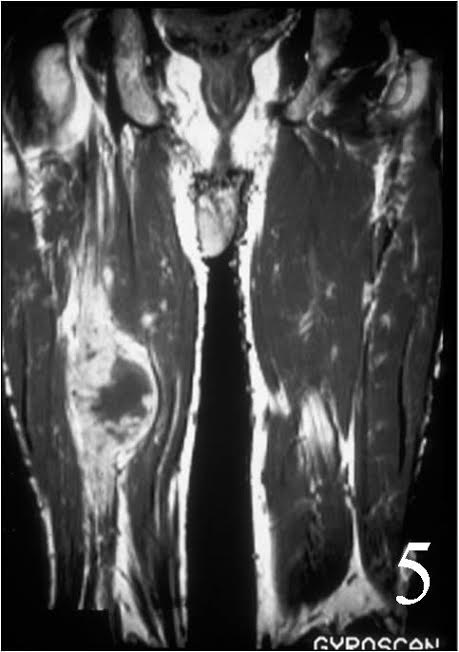
MRI of the thigh, showing a heterogeneous soft tissue lesion in the posterior compartment of the thigh on axial (Fig. 2) and coronal (Fig. 3) T1W images. The addition of gadolinium contrast shows enhancement in the periphery of the mass with necrosis and hemorrhage in the center of the mass typical of a high grade sarcoma (Fig. 4 and 5)
HISTOLOGY
Gross
- Fleshy, white-tan surface marked by areas of secondary hemorrhage and necrosis (Fig. 6)
- Usually large than 5cm in diameter
- Spread of the tumor demonstrated for the thickening of the nerve proximally and distally to the mass. Tumor spread appears as thickening of nerve proximal and distal to the mass
 Fig. 6 Photograph of a gross specimen shows a fleshy, white-tan surface with areas of necrosis and hemorrhage.
Fig. 6 Photograph of a gross specimen shows a fleshy, white-tan surface with areas of necrosis and hemorrhage.
Microscopic
- Resembles fibrosarcomas
- Usually high grade features
- Spindle cells with markedly irregular contours (Fig. 7, 8)
- Nuclei are comma-shaped
- Cells are arranged in sweeping fascicles
- Extensive perineural and intraneural spread
- Proliferation of tumor into subendothelial zone of the vessels
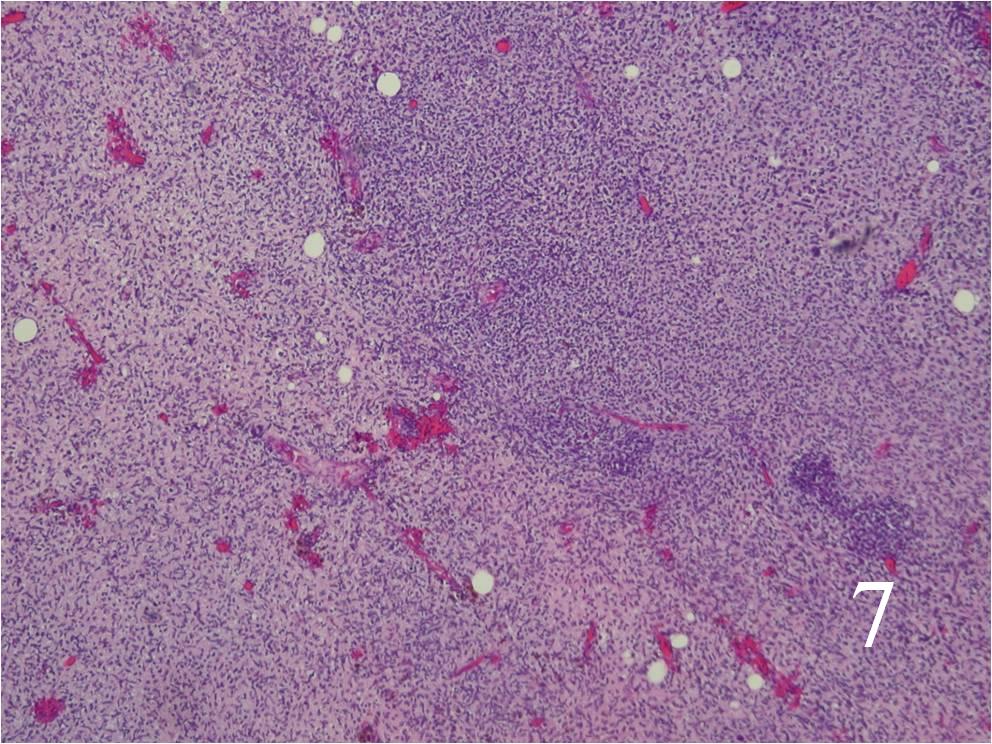
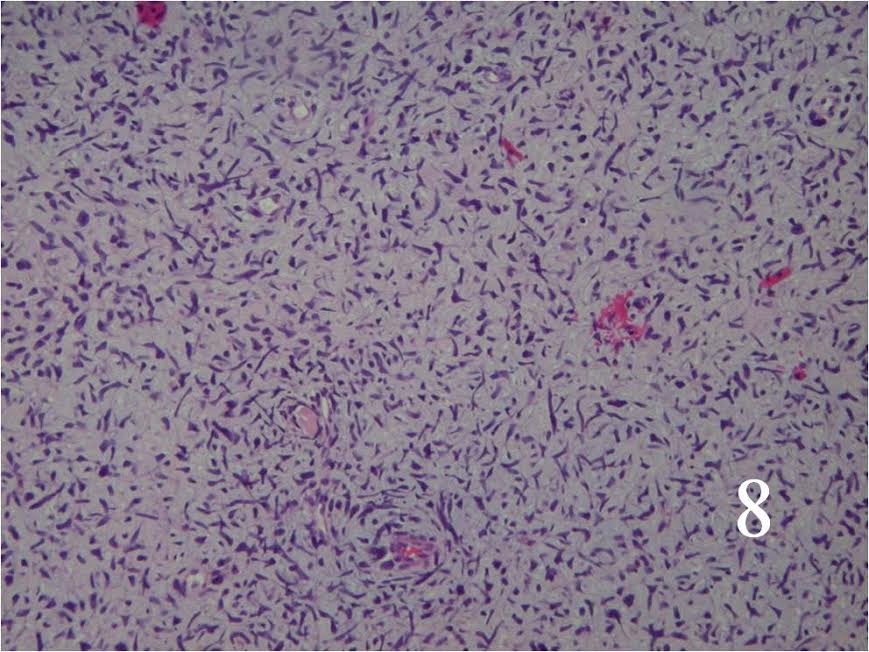 Fig. 7 Low power and high power (Fig. 8) magnification on H&E staining shows a spindle cell neoplasm with high cellularity, abnormal mitotic features and nuclear atypia. The cells are arranged in a somewhat fascicular manner
Fig. 7 Low power and high power (Fig. 8) magnification on H&E staining shows a spindle cell neoplasm with high cellularity, abnormal mitotic features and nuclear atypia. The cells are arranged in a somewhat fascicular manner
Immunohistochemistry
- S-100 protein positive (Fig. 9)
- Vimentin positive
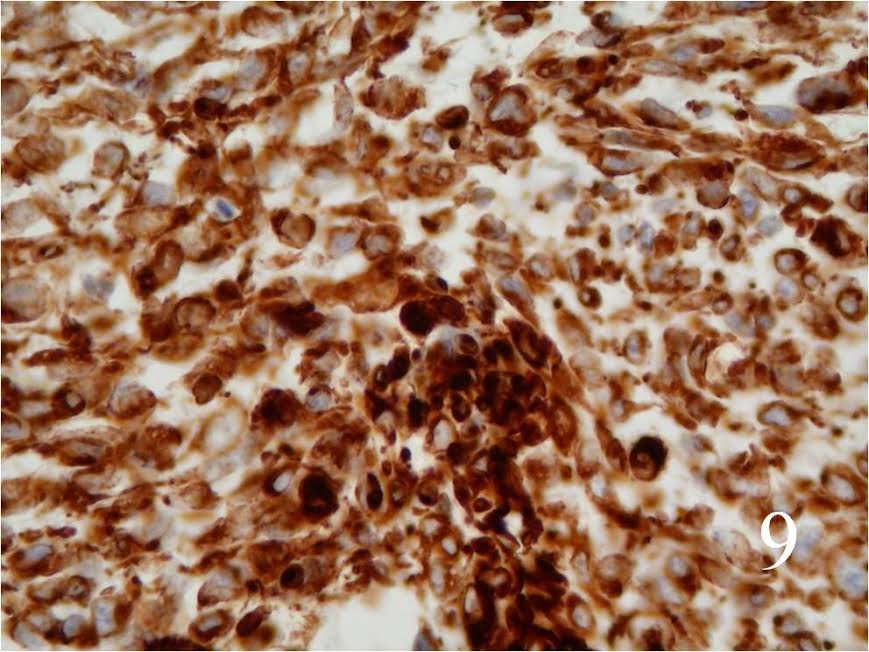 Fig. 9 Positive S-100 staining
Fig. 9 Positive S-100 staining
BIOLOGICAL BEHAVIOR AND PROGNOSIS
- MPNSTs
o Metastases in 65% (to lungs and bones)
o Local recurrence in 40% (difficult to achieve complete excision of the tumor)
- When is associated with NF1, higher risk increase of death . Lower survival rates when associated with NF1
TREATMENT
- Wide resection and postoperative radiation (Fig 10, 11)
- Amputation for unresectable tumor or some cases of recurrence
- Chemotherapy often indicated
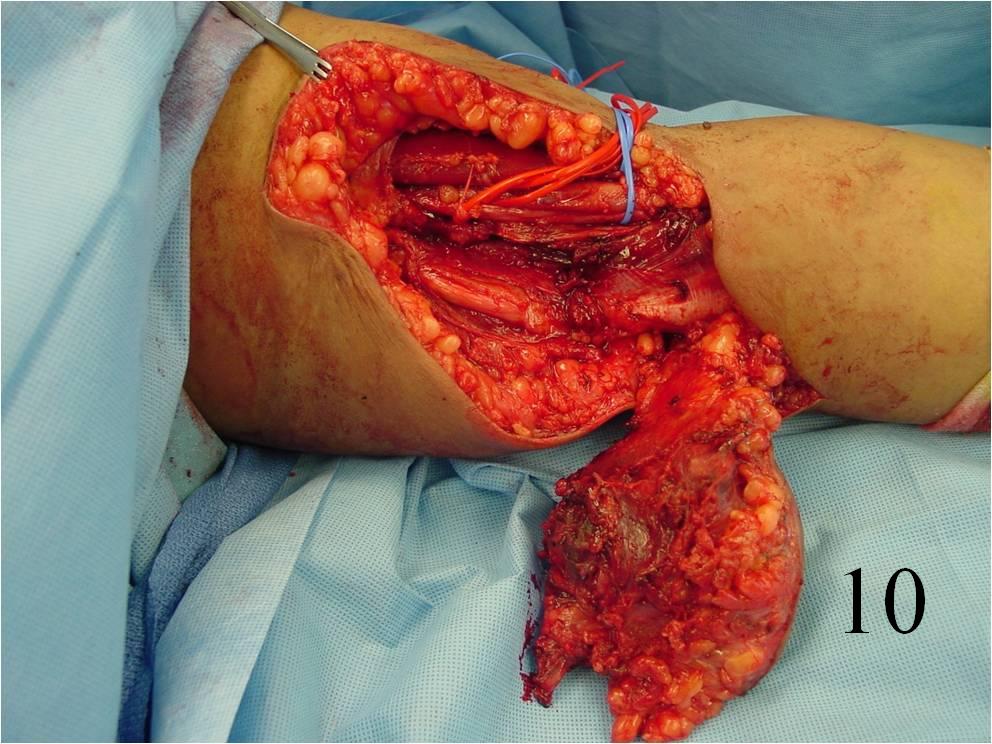
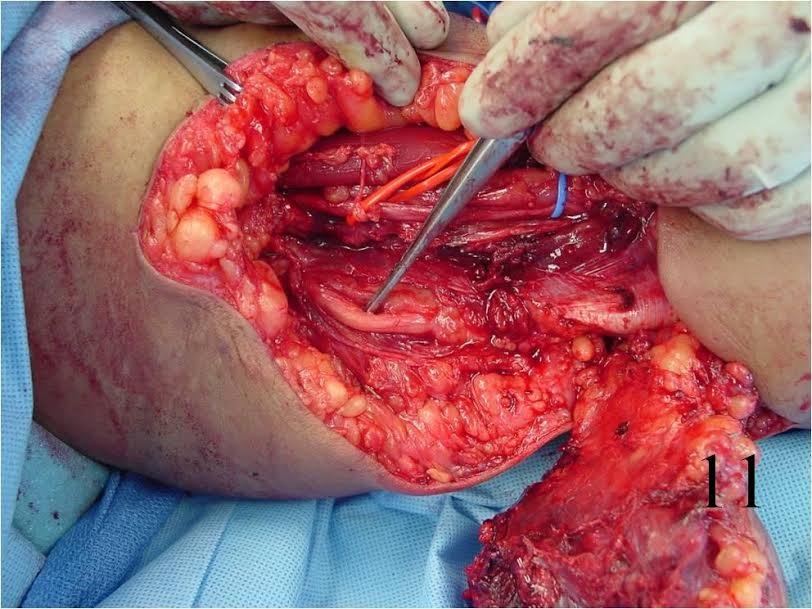 Fig. 10, 11 Intraoperative photographs of a resection of tumor arising in upper extremity.
Fig. 10, 11 Intraoperative photographs of a resection of tumor arising in upper extremity.
