GENERAL INFORMATION
Myositis ossificans is a benign intramuscular mass usually caused by an injury. It can form directly in a muscle or form closely applied to the surface of a bone. Also called benign fibro-osseous lesion or heterotopic ossification is composed of cellular fibrous tissue and metaplastic bone. Myositis ossificans can present as various forms: circumscripta (localized), and progressiva (fibrodysplasia ossificans progressiva). Myositis ossificans can be present also in superficial locations: subcutis, called panniculitis ossificans, and fascia or tendons, called fasciitis ossificans.
CLINICAL DATA
• History of trauma event
• Painless
• Mass with fast growth
DIFFERENTIAL DIAGNOSIS
• Extraskeletal osteosarcoma
• Parosteal osteosarcoma
• Metastatic lesion
CLINICAL PRESENTATION
Signs/Symptoms
• Presents as painless mass but may be paiful
• In young patient usually grows rapidly with a history of trauma
• Almost 75% related to an injury (4 to 8 weeks after trauma)
Age
• Young and active patients
Sites
• Upper extremity
• Hand
• Lower extremity
• Gluteus
• Thigh
RADIOGRAPHIC PRESENTATION
Plain Radiograph
• Periosteal reaction, with thing calcification in the periphery of the lesion (Fig. 1)
• As matures see zonal phenomenon with mature bone at periphery and immature center similar to medullary canal.
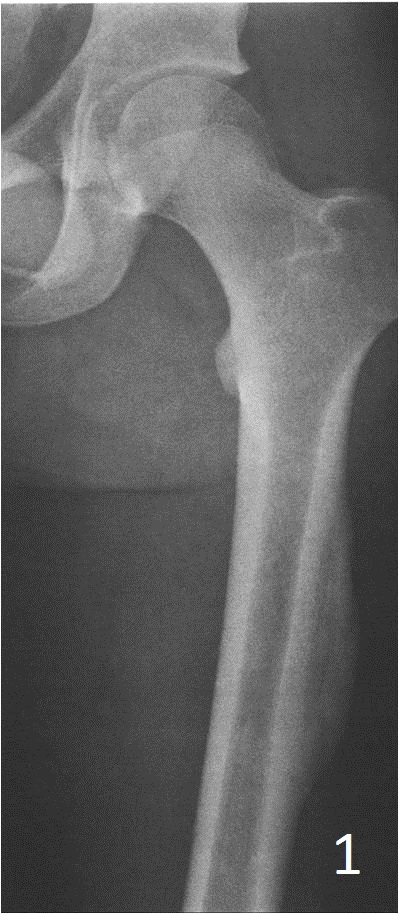
Fig. 1: AP xray of femur shows a periosteal reaction with eggshell calcifiction at the periphery
MRI
• Well defined heterogeneous mass on T1W and IR sequences (Fig. 2, 3) heterogeneous enhancement on postcontrast images (Fig. 4)
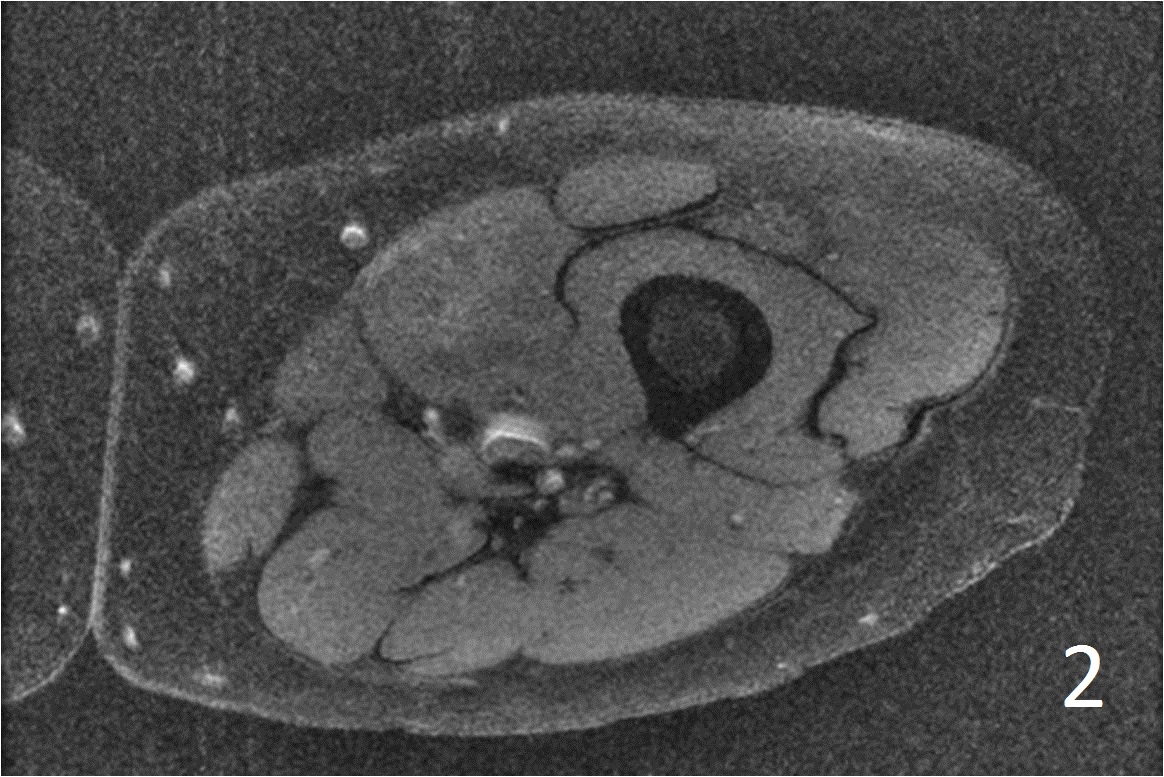
Fig. 2
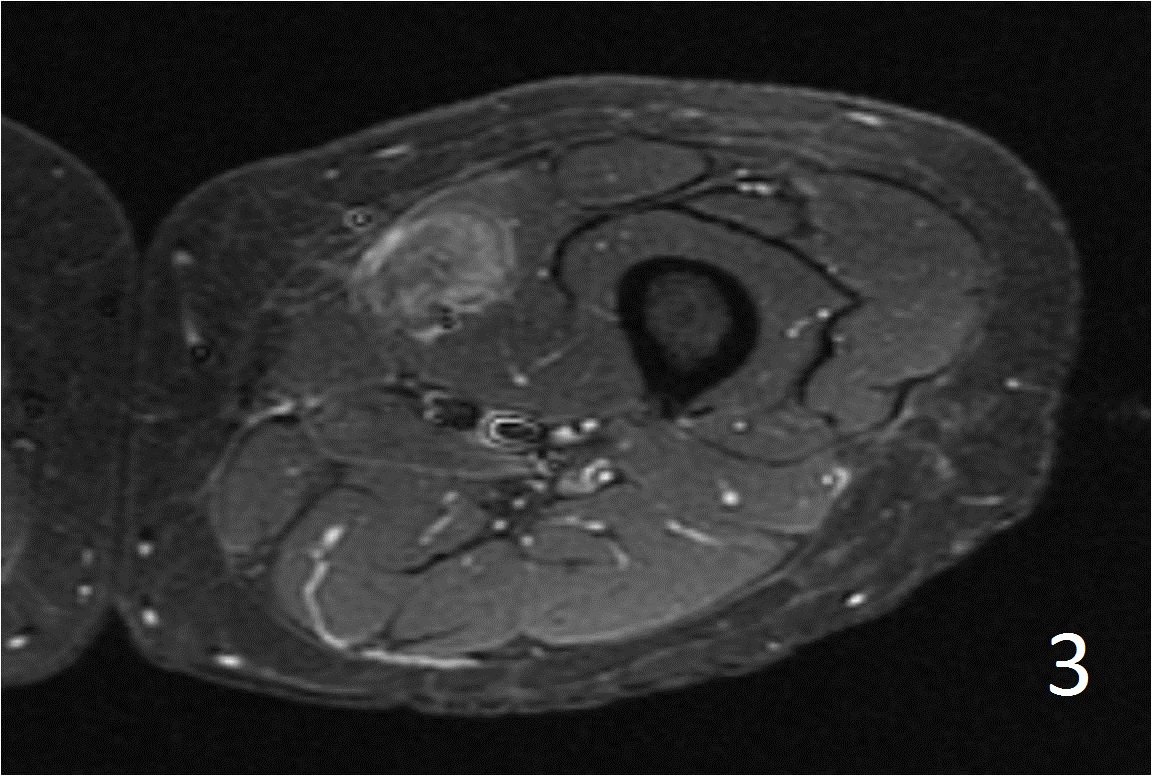
Fig. 3
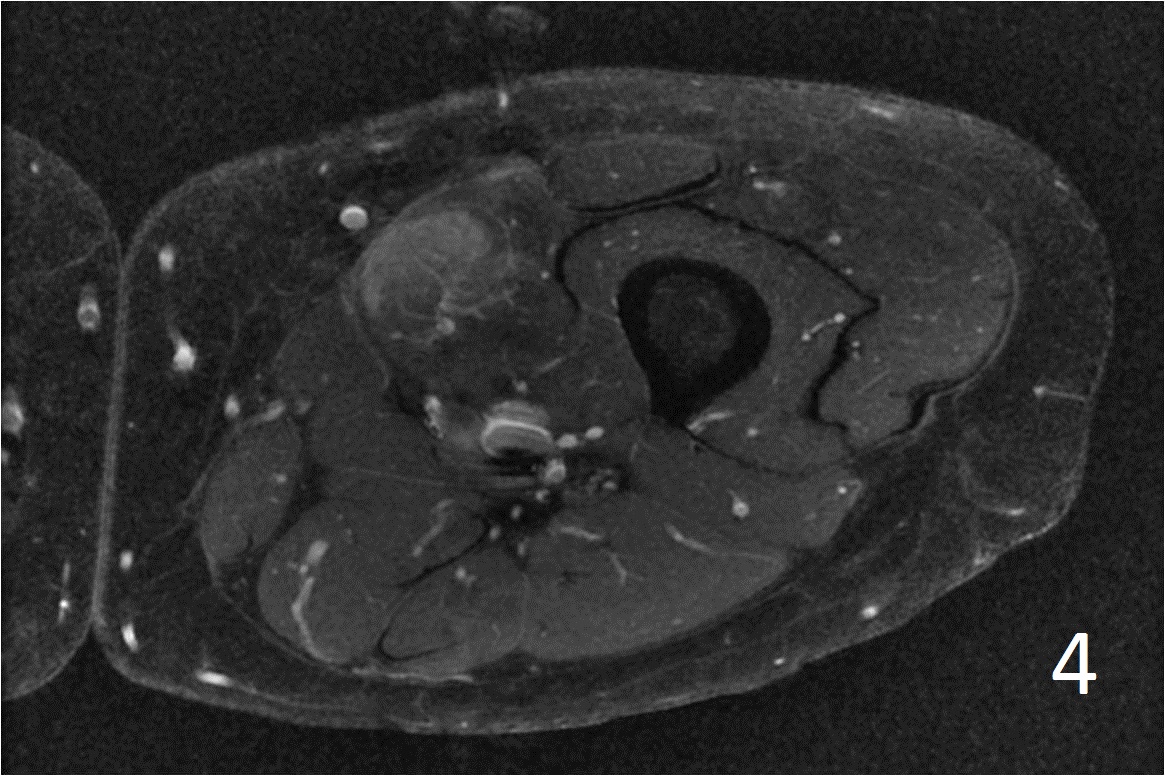
Fig. 4
Fig. 2-4: Axial T1W FS of the thigh shows a ill-defined mass in medial thigh, and fairly well defined and heterogeneous on IR sequence (Fig. 3). Axial T1W displays a heterogeneous mass with mild enhancement post gadolinium (Fig. 4)
PATHOLOGY
Gross
• Well circumscribed lesion
• Has soft core and coarse in the periphery of the mass
Microscopic
• Very cellular stroma combined with immature new bone formation, possible few mitotic figure (Fig. 5, 6, 7)
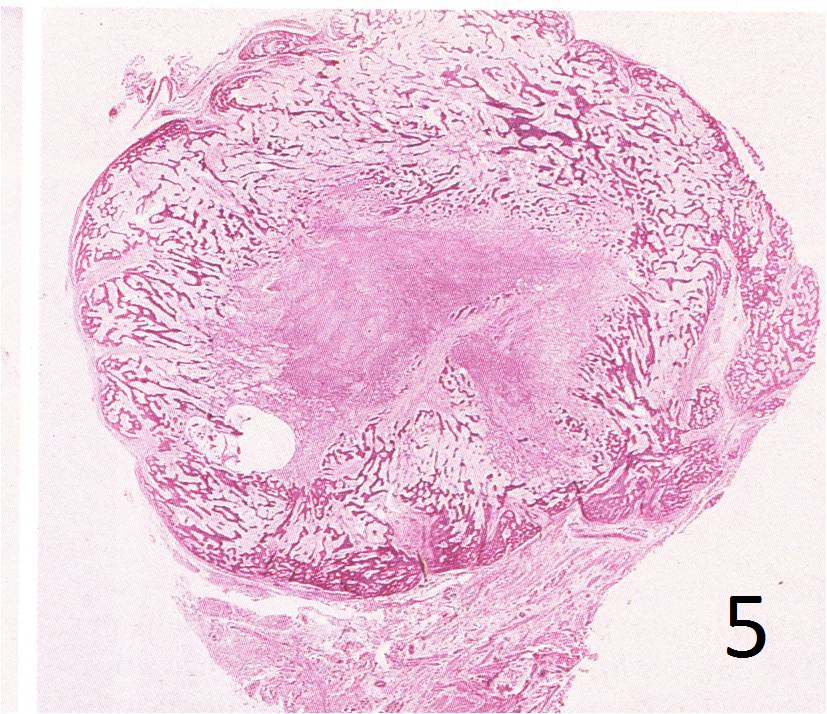
Fig. 5: Microscopic: Low power H & E magnification of lesion, shows a mature bone at the periphery with a central canal forming.
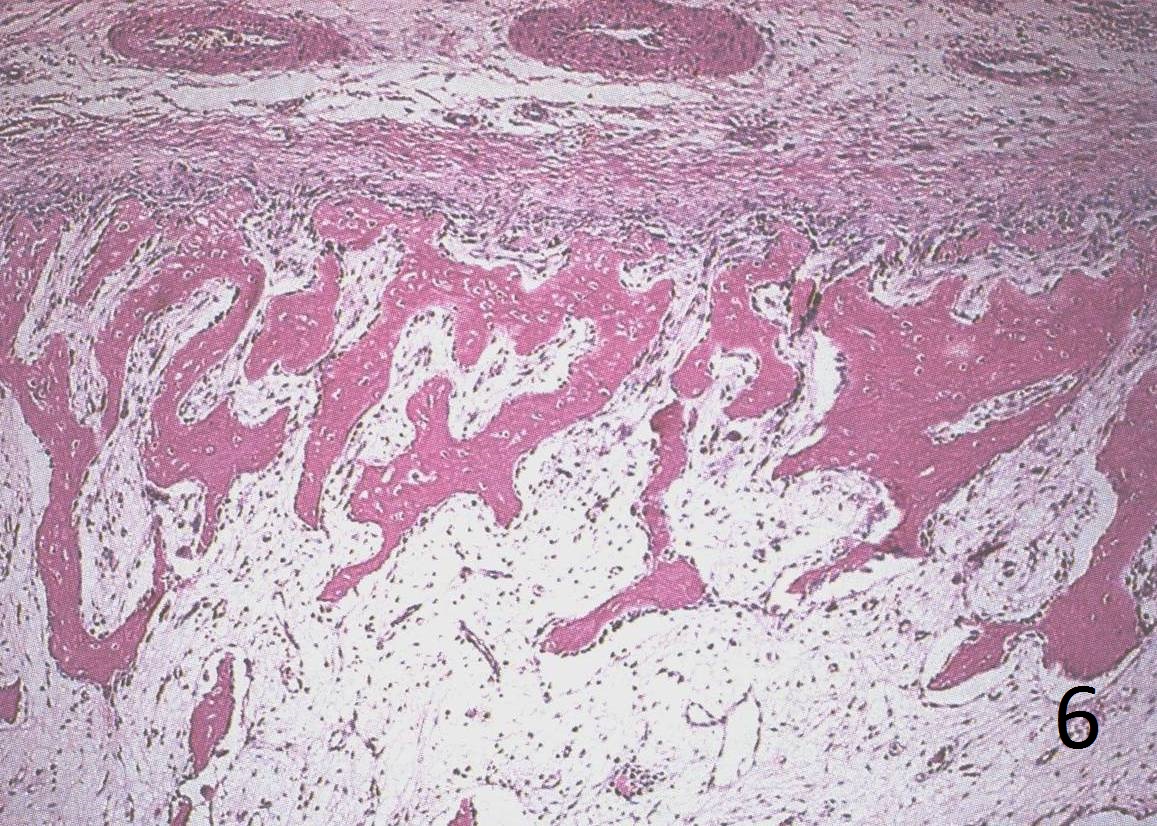
Fig. 6: Low power magnification demonstrates mature bone and fibroblastic cells.
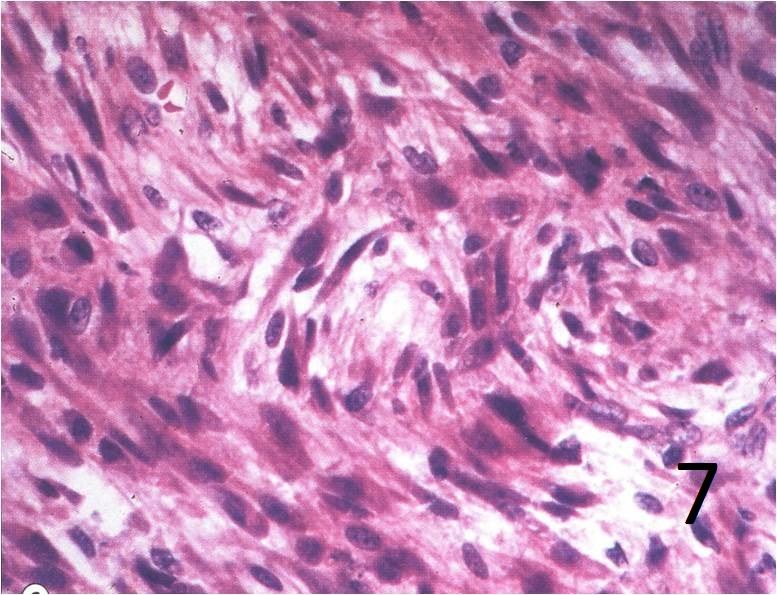
Fig. 7: High power magnification shows uniform fibroblasts, with eosinophilic cytoplasm and variable nuclei, many mitosis but no atypia.
IMMUNOHISTOCHEMICAL
• Vimentin positive
• Actin variable
• Desmin variable
PROGNOSIS
Biological Behavior
• Can mimic a high grade sarcoma, point to take in consideration during the biopsy
• The pathology must be interpreted in conjunction with clinical history and radiological studies.
• Can regress without surgery, close follow-up must to be recommended due resemble sometime high grade sarcomas.
• Extremely rare recurrence after complete excision.
TREATMENT
• Observation until matures based on bone scan turning negative
• Excision for selected symptomatic cases
