GENERAL INFORMATION
Liposarcoma is one of the most commonly diagnosed soft tissue sarcoma, accounting for approximately 12.8% of all sarcomas. Most patients are older than 50 years of age who complain of a large, painless, deep-seated mass located proximally in the extremities. Liposarcoma is a malignant mesenchymal neoplasm composed of lipogenic tissue with varying degrees of atypia. MRI is nonspecific except for well-differentiated tumors in which fat signal is easily distinguished.
Different types of Liposarcoma have been described depending on their histology, including;
well-differentiated liposarcoma (40%), myxoid liposarcoma/round cell liposarcoma (30%), pleomorphic (15%) and dedifferentiated liposarcoma (5%) with different clinical behavior.
Well Differentiated Liposarcoma (WDLPS)
Well-differentiated liposarcoma is the most common subtype of liposarcoma. These tumors nearly always occur in adults and have no gender predilection. They arise most commonly in the deep soft tissues of the proximal extremities (Thigh) and the retroperitoneum. Occasionally retroperitoneal liposarcomas may present as groin masses because of local extension into the peritoneal-lined scrotal sac and therefore may simulate a groin hernia
CLINICAL DATA
Rare; 2 per 1,000,000 habitants
•
Most commonly presents in patients over 50 years old
•
No gender predilection
•
Commonly on deep soft tissue of proximal extremities and retroperitoneum
•
Grows slowly
•
Always deep and never subcutaneous location
•
Do not metastasize
•
Can dedifferentiate into a dedifferentiated liposarcoma (develop a high grade spindle cell component)
DIFFERENTIAL DIAGNOSIS
•
Different types of Liposarcoma
•
Lipoma
•
MFH
•
Synovial Sarcoma
•
Other sarcomas (e.g. fibrosarcomas , other sarcomas (e.g. fibrosarcoma, leiomyosarcoma)
•
Fat containing masses in the retroperitoneum (e.g. angiomyolipoma, myelolipoma)
•
Hibernoma
CLINICAL PRESENTATION
Signs/symptoms
•
Painless enlarging mass
•
Can attain a very large size
•
Locally Aggressive
•
Nonmetastatic tumor
Prevalence
•
No gender prevalence
Age
•
Most cases are diagnosed in the 6th decade.
•
One of the most common soft tissue sarcomas
•
Rare in children.
Sites
•
Lower extremities (50%)
•
Thigh is most common site
•
Retroperitoneum (20%–33%)
•
Upper extremity (14%)
•
Trunk (12%)
RADIOGRAPHIC PRESENTATION
Slow growth
•
Variable sizes, normally more than 10 cms.
•
Thick internal septations
•
Deep location usually intermuscular
CT
Patterns based on amount and distribution of fat:
1.
solid - attenuation > + 20 HU
2.
mixed - areas of < -20 HU and areas of > + 20 HU
3.
pseudocystic - homogenous density between – 20 and + 20 HU
CT findings favoring a liposarcoma from a lipoma include
•
poor definition of adjacent structures
•
nonhomogeneous attenuation, with evidence of significant amounts of soft-tissue within the fatty
mass
MRI (Fig. 1, 2, 3 and 4)
•
Large encapsulated lipomatous mass. (Fig. 1, 2, 3 and 4)
•
Greater than 75% adipose tissue (Hyperintense on T1-weighted) (Fig. 1)
•
Nonadipose components; prominent thick septa and focal nodular regions usually less than 2 cm in size. (Fig. 3)
•
Loss of signal on fat-saturated T1-weighted images.
•
MRI does not appear homogeneous. (Fig. 4)
•
High signal on T1 and low signal on T2 fat suppressed
•
Fibrous stranding typical
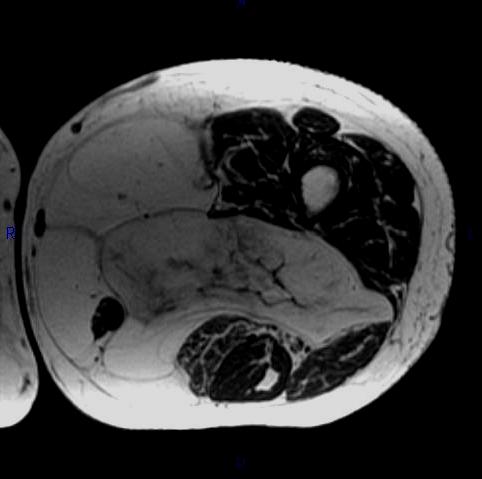 Fig. 1 MRI: Axial T1-weighted (fig1), demonstrates high signal intensity isointense with fat. Intermuscular adypocitic lesion with fatty signal and thickened septa and nodularity
Fig. 1 MRI: Axial T1-weighted (fig1), demonstrates high signal intensity isointense with fat. Intermuscular adypocitic lesion with fatty signal and thickened septa and nodularity
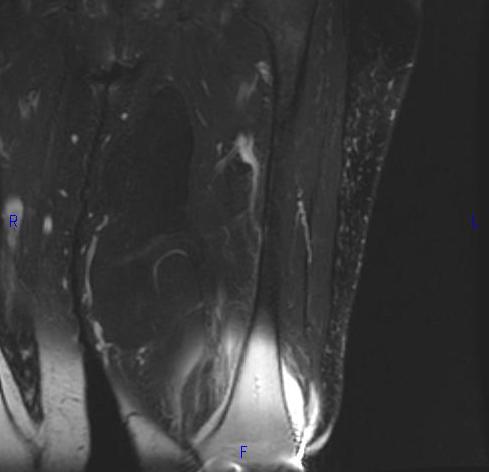 Fig. 2
Fig. 2
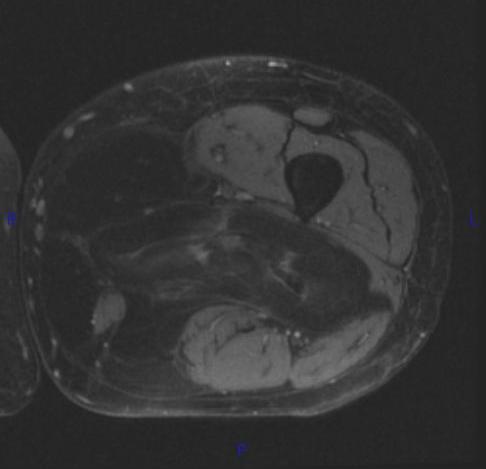 Fig. 3
Fig. 3
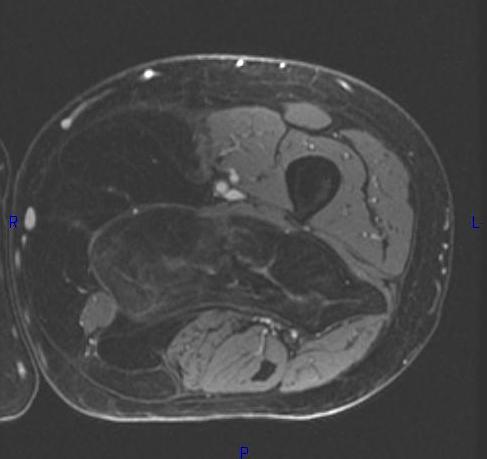 Fig. 2-4 MRI: Coronal T2-weighted fat suppressed (Fig. 2) and Axial T2-weighted FS (Fig. 3) shows low intensity signal isointense with fat. Adypocitic lesion with fatty signal is located in the posterior and medial compartment of the thigh. Thickened septa and nodularity enhances on post contrast images. (Fig. 4)
Fig. 2-4 MRI: Coronal T2-weighted fat suppressed (Fig. 2) and Axial T2-weighted FS (Fig. 3) shows low intensity signal isointense with fat. Adypocitic lesion with fatty signal is located in the posterior and medial compartment of the thigh. Thickened septa and nodularity enhances on post contrast images. (Fig. 4)
PATHOLOGY
Multinodular growth within and between skeletal muscle
•
Soft and pale yellow on cut
 Fig. 5 Gross Pathology. Large lipomatous mass. Well circumscribed and lobulated white-yellow mass. Areas of fat necrosis are common in larger lesions.
Fig. 5 Gross Pathology. Large lipomatous mass. Well circumscribed and lobulated white-yellow mass. Areas of fat necrosis are common in larger lesions.
Microscopic Pathology (Fig. 6, 7, 8)
•
Atypical stromal cells and lipoblasts in the context of mature fat
•
Lipoblasts are immature fat cells often with a bizarre displaced nucleus (the nuclei of benign fat cells are usually very thin and displaced to periphery of cell membrane)
•
Often with a prominent fibrous component
•
The fat cells are often different sizes and shapes
•
Genetic marker and ring chromosomes (12q13-15)
•
Overexpression of oncogenes MDM2 and CDK4 (positive IHC for those markers).
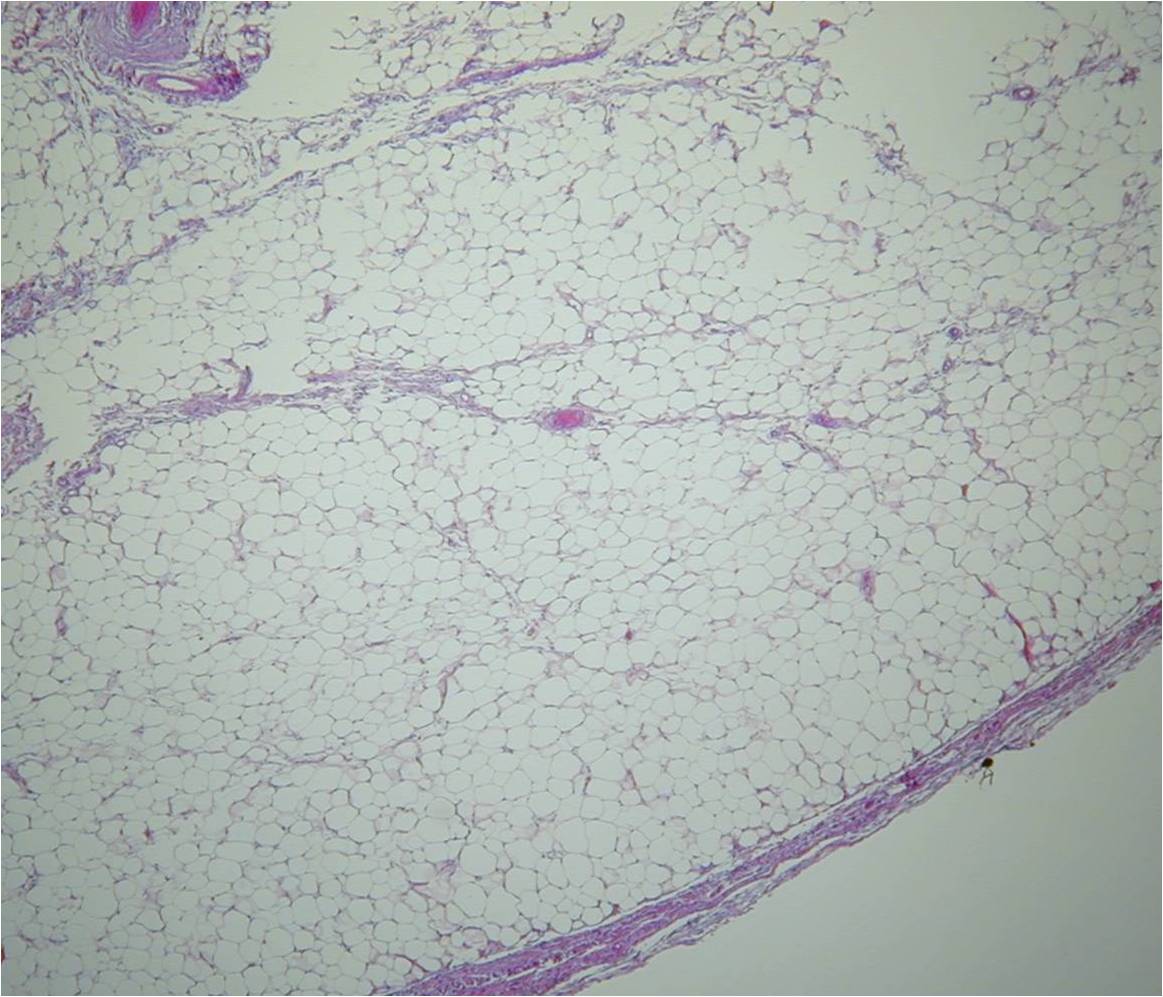
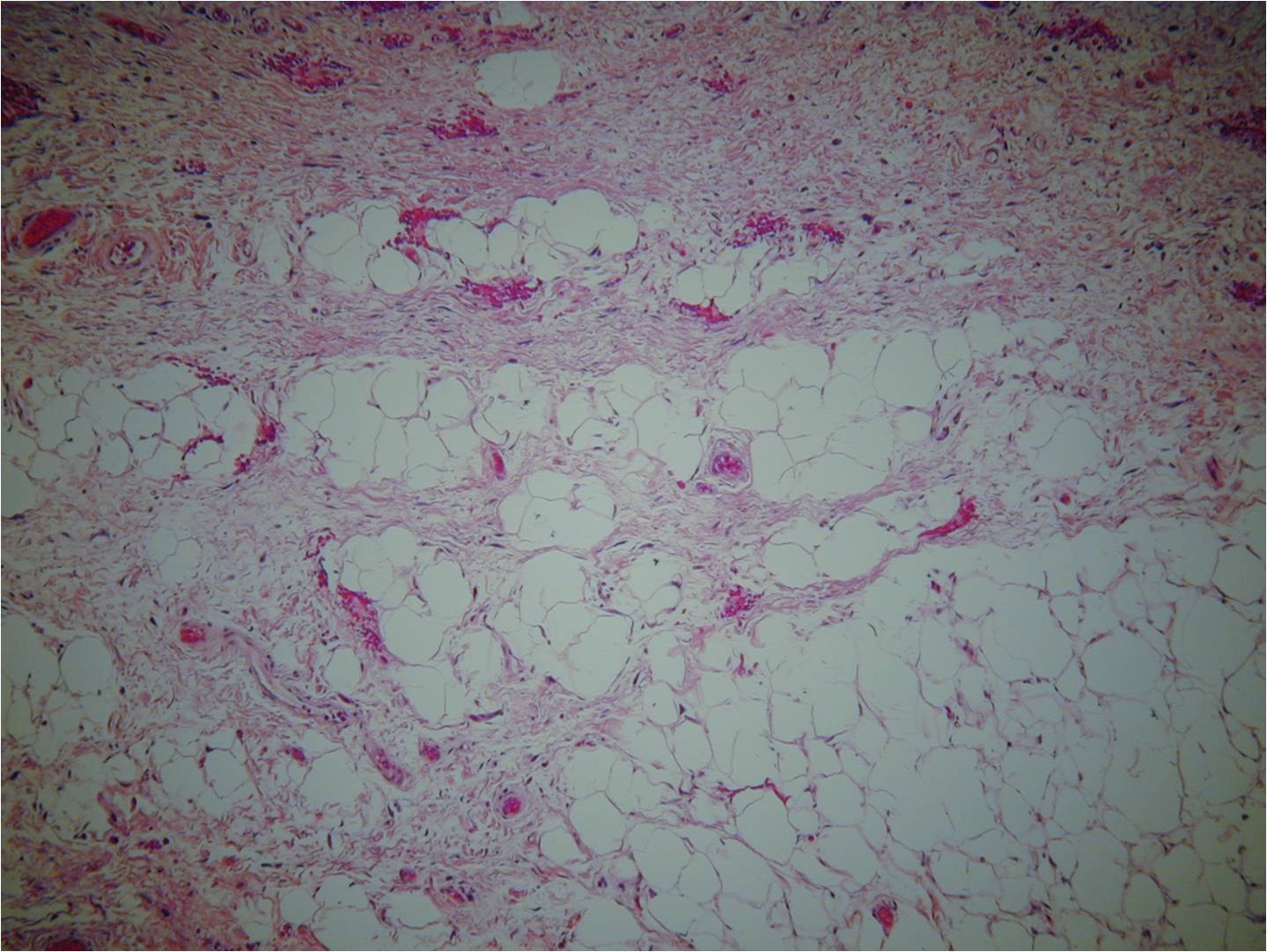
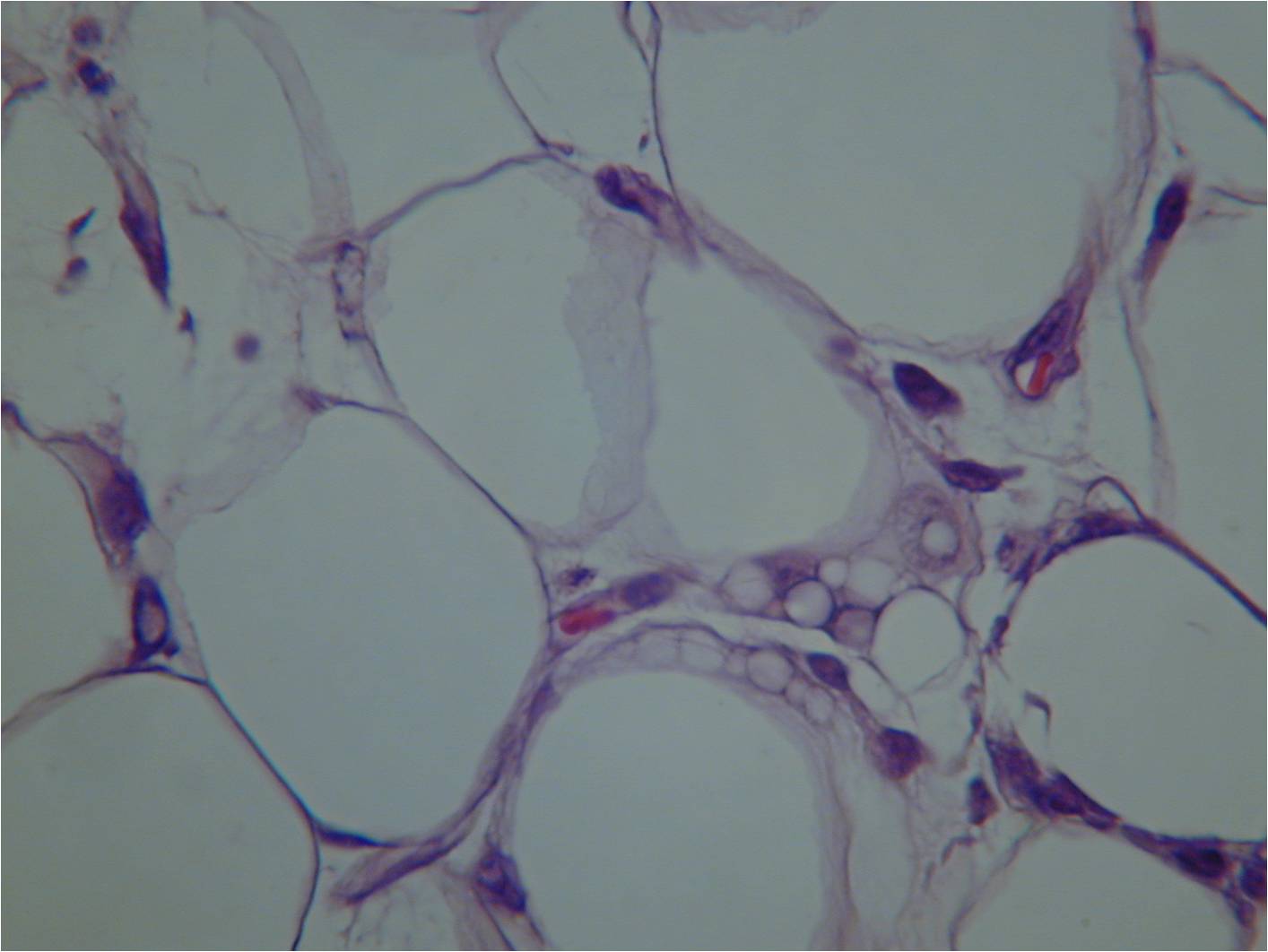 Fig. 6-8 Microscopic Pathology. Low (Fig. 6), medium (Fig. 7) and high (Fig. 8) magnification H & E slides. Atypical stromal cells and lipoblasts in the context of mature fat. Often with a prominent fibrotic component and stranding. Higher magnification shows disorganized stromal cells and hyperchromasia of nuclei.
Fig. 6-8 Microscopic Pathology. Low (Fig. 6), medium (Fig. 7) and high (Fig. 8) magnification H & E slides. Atypical stromal cells and lipoblasts in the context of mature fat. Often with a prominent fibrotic component and stranding. Higher magnification shows disorganized stromal cells and hyperchromasia of nuclei.
PROGNOSIS
Biological behavior
•
Slow growth
•
WDLPS on extremities have shown 95% of disease-specific survival
•
WDLPS on retroperitoneum had an 87% of disease-specific survival
•
Location and margins are the most important prognosis factors.
•
Generally never metastasize
•
Progression to dedifferentiated LPS occurs in 17% of the retroperitoneal WDLPS in the retroperitoneum and 6% for the WDLPS in the extremities.
•
Local recurrence rate depends on size and exact location; 13-46% for WDLPS in the extremities and 91% for the retroperitoneal cases.
TREATMENT
•
Surgery is the mainstay of treatment. The most reliable means of obtaining local tumor control is by surgical excision with a wide excision if possible however most are marginally excised. (Fig. 9-13)
•
Adjuvant radiation therapy is not recommended in patients with WDLS. It is generally not radiosensitive and has a less than 1% risk of distant metastasis. The benefit of radiation does not outweigh the risk
•
Chemotherapy has little role in WDLS. It is a low grade tumor. These tumors are often resistant to standard cytotoxic chemotherapies, and no survival benefit derived from adjuvant chemotherapy have been published.

Fig. 9
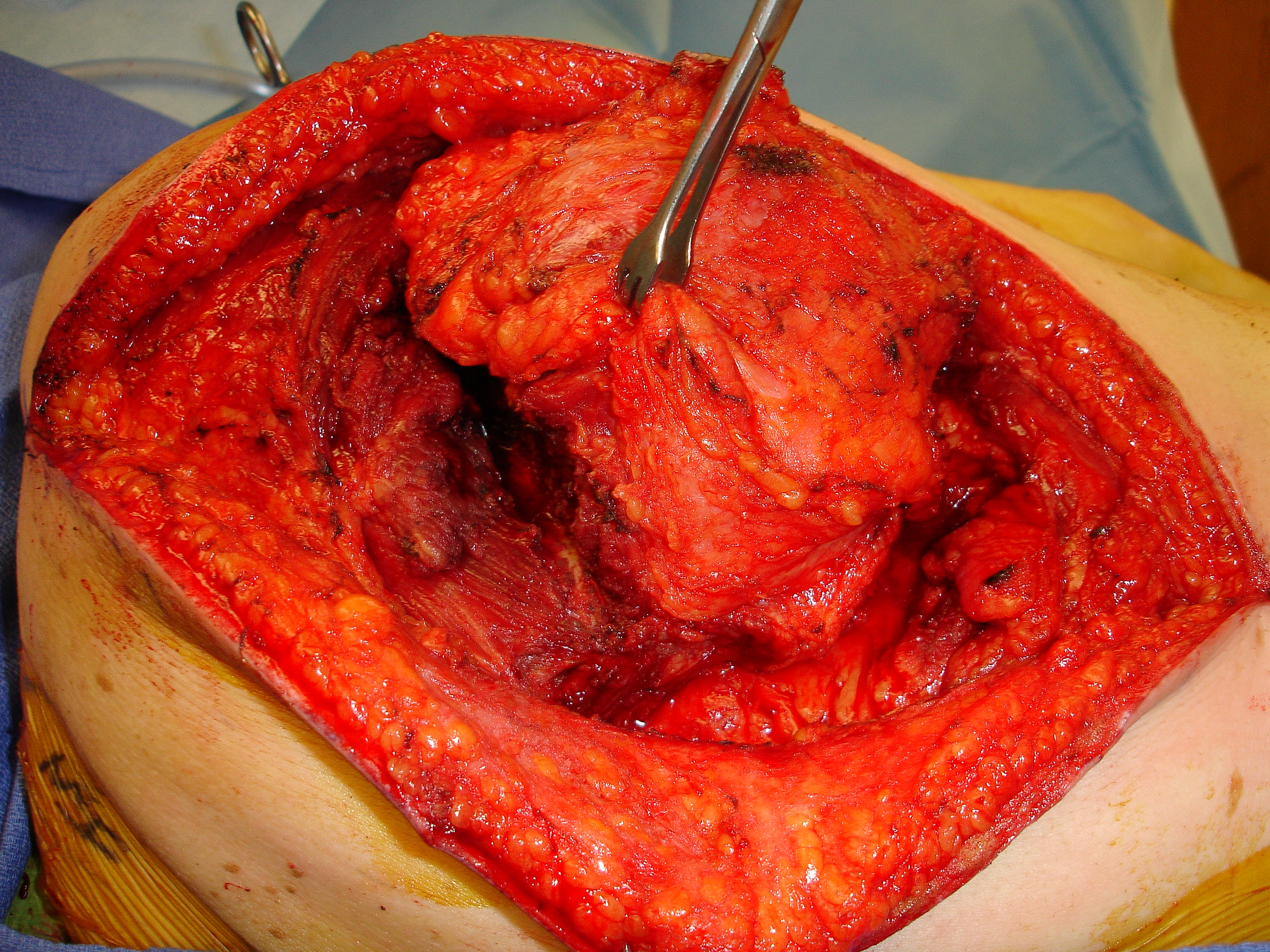
Fig. 10
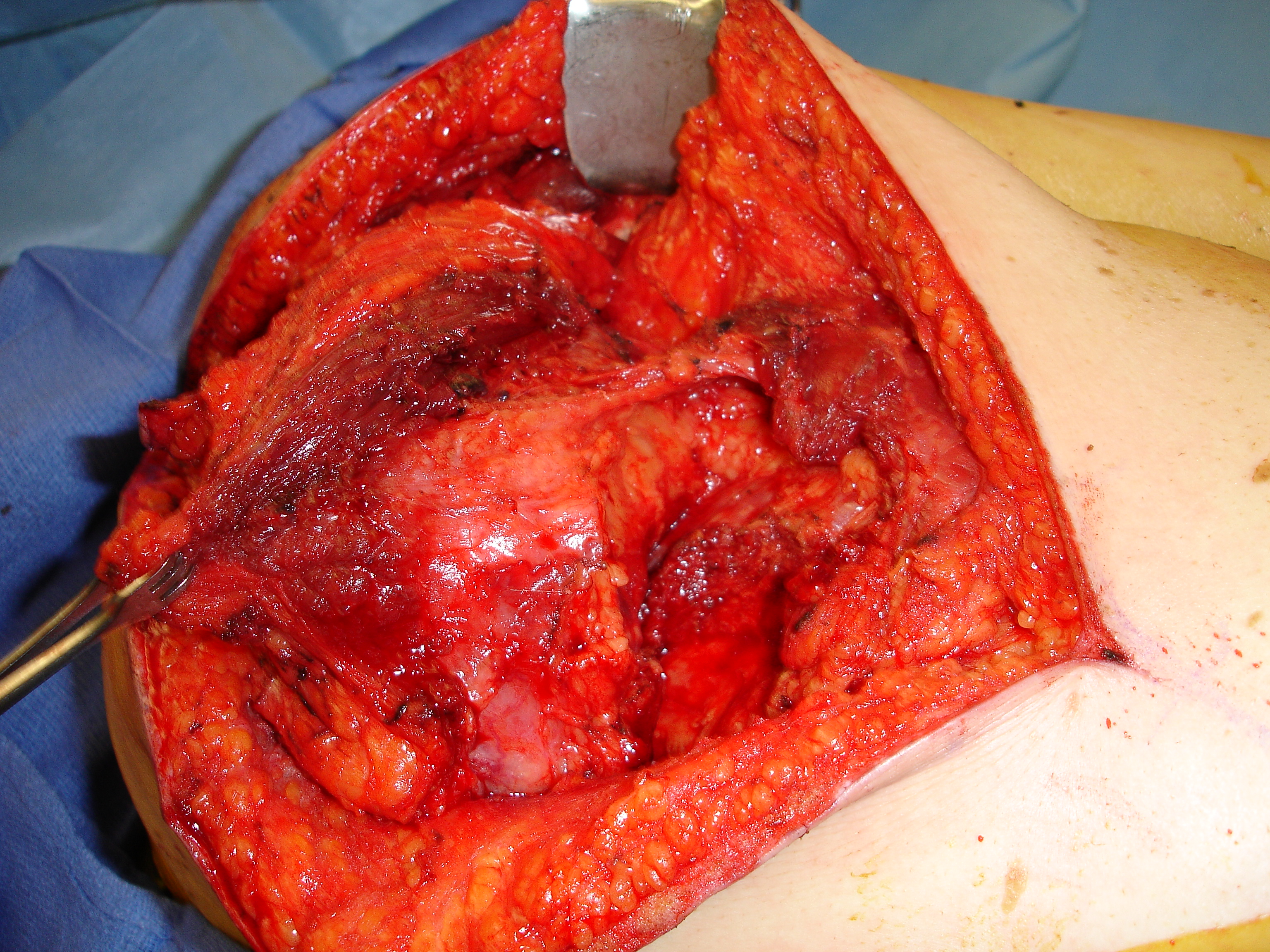
Fig. 11
 Fig. 12
Fig. 12
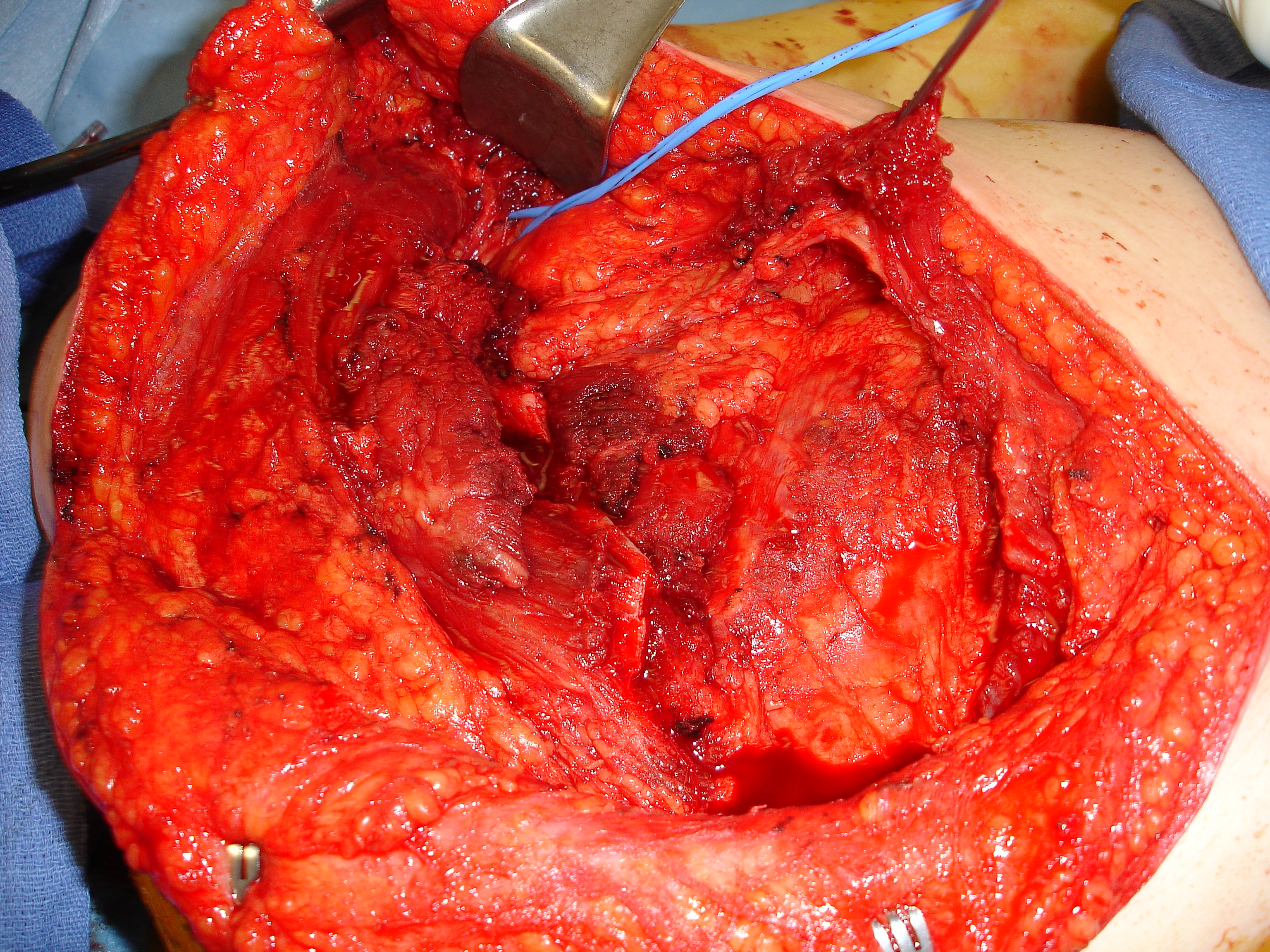 Fig. 13
Fig. 13
Fig. 9-13 Intraoperative. Wide Resection of an intermuscular Well Differentiated Liposarcoma.
